

What Is a Visual Schedule in Autism? A Complete Guide
A visual schedule for autism is one of the most practical, most researched, and most consistently effective tools available for supporting autistic children and adults across home and school settings. If you have been hearing about visual schedules for autism and wondering whether they actually work, how to make one, and whether your child or student genuinely needs one, this post answers all of those questions directly and honestly.
A visual schedule for autism uses images, symbols, photographs, or written words to represent the sequence of activities or tasks in a day or within a specific activity. Rather than relying on verbal instructions that may be difficult to process, retain, or act on, a visual schedule for autism gives the autistic person a concrete, predictable, and independently accessible representation of what is coming next.
This post covers the theory behind why visual schedules for autism work, the research supporting their use, how to build and implement one effectively, and what to do when they are not working as well as you hoped.
Table of Contents
What Is a Visual Schedule for Autism and Why Does It Work
Who Benefits Most From a Visual Schedule for Autism
Types of Visual Schedules for Autism
Visual Schedules for Autism at Different Ages
How to Build a Visual Schedule for Autism at Home
How to Implement a Visual Schedule for Autism at School
Visual Schedules for Autism and Transitions
Common Mistakes With Visual Schedules for Autism
When a Visual Schedule for Autism Is Not Enough
Final Thoughts
What Is a Visual Schedule for Autism and Why Does It Work
A visual schedule for autism works because it addresses several of the core processing differences that characterize autistic neurology simultaneously.
Autistic individuals frequently experience challenges with working memory, which is the ability to hold and manipulate information in the mind over short periods. Verbal instructions, which require the listener to hear, process, retain, and act on spoken information, place significant demands on working memory. For many autistic children and adults, verbal instructions simply do not stay accessible long enough to act on them reliably.
A visual schedule for autism removes the working memory demand by making the information permanently visible and accessible. The autistic person does not need to remember what comes next. They can look at the schedule and see it.
Visual schedules for autism also address the deep autistic need for predictability and routine. Unexpected changes are one of the most consistently distressing experiences for autistic individuals across the spectrum. A visual schedule for autism creates a concrete, visible representation of what the day holds, reducing the uncertainty that drives much of the anxiety and distress that autistic children and adults experience around transitions and unexpected events.
Finally, visual schedules for autism support independence. Rather than needing to ask a teacher or parent what comes next, an autistic child with access to a well-designed visual schedule can navigate transitions and activities with significantly more autonomy, which is both practically beneficial and deeply affirming for a population that often has very little control over their environment.
Who Benefits Most From a Visual Schedule for Autism
Visual schedules for autism are beneficial across the spectrum, but some autistic individuals benefit more immediately and more dramatically than others.
Children and adults who benefit most from a visual schedule for autism include those who:
Struggle significantly with transitions between activities
Experience high anxiety around unexpected changes to routine
Have difficulty following multi-step verbal instructions
Show significant distress at the end of preferred activities
Are working on building independence in daily routines
Have limited or no functional spoken language and rely on visual processing
Visual schedules for autism are not only for young children or for those with significant support needs. Many autistic teenagers and adults use visual schedules and visual planning tools because they genuinely support executive functioning in ways that no amount of effort or willpower can replicate without them.
Types of Visual Schedules for Autism
Visual schedules for autism come in several different formats, and choosing the right one for your specific child or student matters significantly.
Object schedules: For very young children or those with significant support needs, real objects representing each activity can be used. A cup for snack time, a book for reading, a shoe for outdoor time. Object schedules are the most concrete level of visual representation and work well for children who are not yet reliably processing photographs or symbols.
Photograph schedules: Photographs of the actual activities, environments, and materials involved in each part of the day. Photographs are highly concrete and immediately recognizable, making them effective for children who are beginning to process visual representations.
Symbol or picture communication schedules: Standardized symbol systems such as PCS symbols from Boardmaker or Widgit symbols provide a consistent visual language that can be used across home and school settings. These work well for children who have moved beyond needing photographs to recognize activities.
Written schedules: For autistic individuals with functional reading skills, written schedules provide all the same benefits as picture-based schedules with the added efficiency of text.
Digital schedules: Apps and digital tools that provide visual scheduling on tablets or phones are increasingly popular and offer the significant advantage of always being accessible to the individual wherever they are.
Building a Visual Schedule for Autism at Home
How to Build a Visual Schedule for Autism at Home
Building an effective visual schedule for autism at home does not require specialist materials or significant expense. Here is a practical framework:
Step one: Identify the routine you are scheduling
Start with one specific routine rather than the entire day. Morning routines, bedtime routines, and homework sequences are common starting points. A focused visual schedule for autism is more effective than an overwhelming whole-day representation for many children.
Step two: List every step in the routine
Write down every individual step in the routine in sequence. Be more specific than you think you need to be. Get dressed is not one step. It is underwear, then socks, then trousers, then shirt, then shoes.
Step three: Choose the right visual format
Match the visual format to your child's current level of visual processing. Start concrete with photographs or objects if unsure, and move toward symbols or text as understanding develops.
Step four: Present the schedule at the start of the routine
Go through the visual schedule for autism with your child before the routine begins, pointing to each step in sequence. This primes the brain for what is coming rather than introducing each step as a surprise.
Step five: Allow the child to interact with the schedule
Where possible, allow the child to move or check off completed items on the visual schedule for autism. This interaction with the schedule increases engagement and reinforces the connection between the visual representation and the actual activity.
Navigating the practicalities of implementing tools like visual schedules for autism at home, alongside all the other demands of raising an autistic child, is genuinely challenging and the learning curve is real. Dropped in a Maze by Sonia Chand is the book that so many parents wish had existed when they were starting out, an honest, practical account of navigating the autism journey without a map.
Visual Schedules for Autism at Different Ages
Visual schedules for autism are not only for young children and their benefits extend across the lifespan.
For toddlers and preschoolers, object and photograph schedules support the development of routine understanding and transition compliance during the most developmentally sensitive period for establishing predictable structure.
For school-age children, visual schedules support academic task completion, homework routines, and the increasingly complex social and academic schedule of the school day.
For teenagers, visual scheduling tools support executive functioning, homework management, and the self-directed organization that secondary school increasingly demands.
For autistic adults, visual planning tools including apps, written schedules, and structured daily planners serve the same fundamental function, reducing the cognitive load of executive functioning and making the day more predictable and more manageable.
If you are an autistic adult who has discovered that visual scheduling tools genuinely help you, or a parent supporting an autistic teenager who is developing their own organizational strategies, coaching with Sonia offers personalised support for building the practical life management tools that work with your specific neurology rather than against it.
Book a coaching session with Sonia here and get personalised support for building the daily structure that actually works for your brain.
How to Implement a Visual Schedule for Autism at School
Implementing a visual schedule for autism in a school setting involves several additional considerations beyond the home implementation framework.
Consistency across adults: Every adult who works with the child needs to use the visual schedule for autism in the same way. Inconsistency in how the schedule is presented or referenced significantly reduces its effectiveness.
Placement: The visual schedule for autism needs to be placed where the child can independently access and reference it throughout the day. A schedule that lives on the teacher's desk is not independently accessible and defeats one of the primary purposes of the tool.
Previewing transitions: Before each transition, direct the child's attention to the visual schedule for autism to preview what is coming next. This brief preview significantly reduces transition-related distress because the change is no longer unexpected.
Incorporating the child's input: Where possible, involve the autistic child in building and maintaining their visual schedule for autism. Children who have some ownership of their schedule engage with it more reliably than those for whom it is simply imposed.
Including preferred activities: A visual schedule for autism that includes only demands and transitions and no preferred activities does not accurately represent the day and reduces the child's trust in it. Including preferred activities in the schedule is essential for the tool to function as a reliable predictor of the day.
For educators who want to go deeper into what genuine autism support looks like in a school setting, the On the Spectrum podcast with Sonia Chand covers these practical, real-world topics in honest and accessible conversations that are valuable for educators as well as families.
Listen to the On the Spectrum podcast here and find the insights that help you support autistic students more effectively in your classroom.
Visual Schedules for Autism and Transitions
Transitions are one of the most reliably difficult aspects of daily life for autistic individuals, and visual schedules for autism are one of the most effective tools for reducing transition-related distress.
The distress autistic people experience around transitions is not primarily about the activity that is ending or the activity that is beginning. It is about unpredictability. The autistic nervous system experiences unexpected change as a threat, and the anxiety that follows is a genuine threat response rather than willful non-compliance.
A visual schedule for autism addresses this directly by making the next activity visible before the transition begins. The child who can see that outdoor play is followed by snack, which is followed by circle time, is experiencing a fundamentally different psychological situation than the child who never knows what is coming next.
For autistic children who are particularly demand-avoidant, combining the visual schedule for autism with the indirect language approaches covered in the pathological demand avoidance language to use post can significantly improve transition compliance and reduce the distress associated with necessary routine changes.
Common Mistakes With Visual Schedules for Autism
Even well-intentioned implementation of a visual schedule for autism can fall short if some common mistakes are not avoided.
Making the schedule too complex: A visual schedule for autism that represents an entire day in minute-by-minute detail can be overwhelming rather than clarifying. Start with the key anchor points in the day and add detail gradually.
Not using it consistently: A visual schedule for autism that is only brought out during difficult moments rather than used consistently throughout the day loses its predictive function. The schedule needs to be a regular, reliable part of the routine rather than an emergency intervention.
Not updating it when changes occur: When the schedule genuinely needs to change, updating the visual schedule for autism and previewing the change with the child is essential. The schedule is only a reliable predictor if it actually reflects what is going to happen.
Removing the schedule too quickly: Many parents and educators introduce a visual schedule for autism and then remove it as soon as the child seems to have learned the routine. The schedule is not just a learning tool. It is an ongoing support that reduces the cognitive and anxiety load even for routines that are well established.
When a Visual Schedule for Autism Is Not Enough
A visual schedule for autism is a powerful tool but it is not a complete solution on its own.
When a visual schedule for autism does not seem to be helping, the most common reasons include the format not matching the child's current visual processing level, the schedule not being used consistently across environments and adults, the schedule not including enough preferred activities to be genuinely representative of the day, or the underlying anxiety or sensory load being too high for any single tool to address adequately.
In these cases, a visual schedule for autism is most effective as part of a broader support plan that also addresses communication, sensory needs, and the specific anxiety triggers that are driving the distress.
For a deeper understanding of how different autism support tools and strategies fit together into a comprehensive picture, the post onwhat is level 2 autism covers the kind of multi-domain support planning that complex autism profiles require.
Final Thoughts
A visual schedule for autism is not a complicated or expensive intervention. It is a straightforward, evidence-based tool that works by meeting the autistic brain where it actually is, providing the predictability, the visual processing support, and the independence that autistic individuals consistently benefit from.
Getting it right takes some thoughtfulness in design and consistency in implementation. But when those elements are in place, the difference a visual schedule for autism makes to daily functioning, transition compliance, and anxiety levels is real, measurable, and often significant.
Start simple. Stay consistent. And trust the research that has been building the evidence for this tool for decades.
Is Autism a Learning Disability? What Parents and Adults Need to Know
Is autism a learning disability is one of those questions that gets asked constantly and answered inconsistently, leaving parents and autistic adults more confused than when they started. Is autism a learning disability in the clinical sense? Is it a learning disability in the school system sense? And does the answer even matter practically for getting the right support?
It matters enormously. And the answer is more nuanced than a simple yes or no.
This post answers is autism a learning disability directly and completely, explains what both terms actually mean, covers where they overlap and where they do not, and gives parents and autistic adults the clarity they need to advocate effectively for the right support in the right settings.
Table of Contents
Is Autism a Learning Disability? The Direct Answer
What Is a Learning Disability?
What Is Autism?
Where Autism and Learning Disabilities Overlap
Where Autism and Learning Disabilities Differ
Is Autism a Learning Disability in the US Education System?
How Autism Affects Learning
Co-occurring Learning Disabilities in Autism
What This Means for Educational Support
FAQs
Final Thoughts
Is Autism a Learning Disability?
Is autism a learning disability? In the United States clinical and educational framework, no. Autism and learning disabilities are two separate categories. They can and frequently do co-occur in the same person, but autism is not classified as a learning disability and having an autism diagnosis does not mean a person has a learning disability.
Is autism a learning disability in the UK? This is where the terminology gets genuinely confusing, because in the UK the term learning disability is used to mean something significantly different from what it means in the US. In the UK, learning disability refers to what Americans would call intellectual disability, a significant limitation in intellectual functioning and adaptive behavior. In the US, a learning disability refers specifically to neurological conditions that affect how a person processes information in specific academic areas, such as dyslexia, dysgraphia, or dyscalculia, without necessarily affecting overall intelligence.
Is autism a learning disability therefore depends significantly on which country's framework and which definition of the term you are working within, which is part of why the question generates so much confusion.
This post uses the US definition throughout unless otherwise specified.
What Is a Learning Disability?
Before going deeper into is autism a learning disability, it is worth being precise about what a learning disability actually means in the US context.
In the United States, a learning disability is a neurological condition that affects how the brain processes, stores, and communicates information in specific academic domains. Learning disabilities do not reflect overall intelligence. A person can have a high IQ and significant learning disabilities simultaneously.
The most commonly recognized learning disabilities include:
Dyslexia, which affects reading and language processing
Dysgraphia, which affects writing and fine motor coordination for written tasks
Dyscalculia, which affects mathematical processing and number sense
Auditory processing disorder, which affects how the brain processes sounds
Language processing disorder, which affects understanding and producing language
What these conditions share is that they represent a significant discrepancy between overall cognitive ability and performance in specific academic areas, driven by differences in how the brain processes specific types of information.
Under the Individuals with Disabilities Education Act, known as IDEA, specific learning disability is one of the thirteen disability categories that can qualify a child for special education services. Autism is a separate category under IDEA.
What Is Autism?
Is autism a learning disability requires equal clarity about what autism actually is.
Autism, formally known as Autism Spectrum Disorder or ASD, is a neurodevelopmental condition characterized by differences in social communication, sensory processing, and restricted or repetitive patterns of behavior and interests. It is present from birth and it is lifelong.
Autism does not inherently involve difficulties in specific academic processing areas in the way that learning disabilities do. Autism involves a broader neurodevelopmental profile that affects social communication, sensory experience, and behavioral patterns across all of life, not just in academic domains.
Intellectual ability in autism spans the full range from significant intellectual disability to exceptional cognitive gifts. Many autistic people are highly intelligent academically. Others have average intelligence. Some have intellectual disabilities that affect learning broadly. None of these variations are definitional features of autism itself.
For a comprehensive look at the relationship between autism and intellectual ability specifically, the post onis autism an intellectual disability covers this distinction in full detail.
Where Autism and Learning Disabilities Overlap
While is autism a learning disability has a clear no answer in the US clinical framework, autism and learning disabilities overlap in several practically important ways.
They can co-occur: Research consistently shows that learning disabilities occur at higher rates in autistic individuals than in the general population. Studies suggest that between 30 and 50 percent of autistic individuals have at least one co-occurring specific learning disability. Dyslexia and dysgraphia are particularly commonly co-occurring with autism.
They both affect learning: Both autism and learning disabilities can significantly affect how a person learns, though through different mechanisms. Autism affects learning through social communication differences, sensory processing differences, and executive functioning challenges. Learning disabilities affect learning through specific processing difficulties in defined academic domains.
They both qualify for educational support: Both autism and specific learning disabilities can qualify children for Individualized Education Programs under IDEA and for accommodations under Section 504 of the Rehabilitation Act. When they co-occur, educational planning needs to address both profiles.
They are both neurodevelopmental: Both autism and learning disabilities are classified as neurodevelopmental conditions, meaning they originate in differences in brain development during the early years of life and are present from birth.
Where Autism and Learning Disabilities Differ
Understanding where autism and learning disabilities differ is just as important as understanding where they overlap.
Scope: Learning disabilities affect specific academic processing areas while leaving other areas of cognitive functioning intact. Autism is a broader neurodevelopmental profile that affects social communication, sensory processing, and behavioral patterns across all domains of life, not just academic ones.
Social communication: Social communication differences are a core defining feature of autism and are not a feature of learning disabilities. A person with dyslexia, for example, does not necessarily experience any social communication difficulties at all.
Sensory processing: Significant sensory processing differences are characteristic of autism and are not part of the definition of learning disabilities.
Intelligence: Specific learning disabilities are defined partly by the presence of average or above average intelligence alongside specific processing difficulties. Autism is not defined by any particular level of intelligence and occurs across the full cognitive range.
Is Autism a Learning Disability in the US Education System?
In the US education system, is autism a learning disability in terms of how it is classified under federal law? No.
Under IDEA, autism is listed as one of thirteen separate disability categories that can qualify a child for special education services. Specific learning disability is a separate category. A child can qualify for special education under the autism category, the specific learning disability category, or both, if both profiles are present and both affect educational functioning.
This matters practically because the category under which a child is identified can affect what services and supports are made available to them. A child identified only under specific learning disability may not receive the social communication support, sensory accommodation, and behavioral support that an autism identification would prompt. A child identified only under autism may not receive the specific academic intervention that a learning disability identification would prompt.
When both autism and learning disabilities are present, advocating for identification and support under both categories is often the most effective approach for ensuring the child receives comprehensive educational support.
How Autism Affects Learning
Even though is autism a learning disability has a no answer in the US clinical framework, autism absolutely does affect learning in ways that are practically significant in educational settings.
Autism affects learning through several specific mechanisms:
Executive functioning: Many autistic individuals experience challenges with executive functioning including planning, organization, task initiation, working memory, and cognitive flexibility. These challenges can significantly affect academic performance independently of any specific learning disability.
Sensory processing: Sensory sensitivities can make the physical environment of a classroom genuinely difficult to learn in. Fluorescent lighting, background noise, and physical proximity to other students can all create a sensory load that significantly reduces the cognitive resources available for learning.
Social communication: The social dimension of learning, including group work, classroom discussion, and teacher-student interaction, can be significantly more demanding for autistic students than for neurotypical peers, creating an additional cognitive and emotional load that affects academic performance.
Anxiety: High rates of anxiety in autistic individuals, driven by social demands, sensory environment, and the unpredictability of school settings, significantly affect the ability to access learning even when cognitive ability is intact.
None of these are specific learning disabilities in the clinical sense. But all of them affect learning in ways that require educational accommodation and support.
Navigating the school system and understanding which of these factors are affecting your child's learning is genuinely complex, and having the right support alongside that navigation makes a real difference.
Dropped in a Maze by Sonia Chand is the book that helps families make sense of the autism journey, including the educational piece, in a way that is honest, practical, and grounded in real experience rather than clinical abstraction.

Co-occurring Learning Disabilities in Autism
Because co-occurring learning disabilities are common in autism, understanding how to identify and address them is a practically important part of comprehensive autism support.
Research published in the Journal of Learning Disabilities found that autistic children showed significantly higher rates of reading difficulties, including dyslexia, than the general population, with estimates suggesting that between 20 and 50 percent of autistic children may have co-occurring reading difficulties.
Dysgraphia, which affects written expression, is also commonly co-occurring with autism and is frequently underidentified because the writing difficulties are attributed to the autism rather than being recognized as a separate and specifically addressable condition.
When a learning disability co-occurs with autism, it requires targeted intervention specific to the learning disability alongside the broader autism support. Addressing the autism alone will not resolve a specific learning disability, and addressing only the learning disability will not address the broader autism support needs.
A comprehensive educational assessment that specifically looks for learning disabilities alongside the autism profile is therefore an important step for any autistic child who is struggling academically beyond what would be expected from the autism alone.
For parents navigating the process of getting their child properly assessed, The On the Spectrum podcast with Sonia Chand covers the real, practical challenges of navigating educational systems as an autism family, with honest conversations that give you the information and the community to keep going when the system makes it hard.
Listen to the On the Spectrum podcast here and find the support that helps you advocate more effectively for your child's educational needs.
What This Means for Educational Support
The practical implications of is autism a learning disability for educational support planning are significant.
An autistic child without co-occurring learning disabilities needs educational support that addresses social communication differences, sensory accommodation, executive functioning support, and behavioral regulation, but does not necessarily need the specific academic intervention that a learning disability would require.
An autistic child with co-occurring learning disabilities needs all of the above plus targeted intervention for the specific learning disability. Dyslexia-specific reading intervention for an autistic child with dyslexia, for example, is genuinely different from and in addition to the broader literacy support that autism alone might require.
Getting this right in an IEP requires a comprehensive assessment that specifically looks for both profiles and educational planning that addresses both clearly and specifically. Advocating for that level of comprehensive assessment is one of the most important things parents can do for an autistic child who is struggling academically.
FAQs
Is autism a learning disability?
No. In the US clinical and educational framework, autism and learning disabilities are separate categories. They can co-occur but autism is not classified as a learning disability.
Can you have autism and a learning disability?
Yes. Research suggests between 30 and 50 percent of autistic individuals have at least one co-occurring specific learning disability.
Does autism affect learning?
Yes, through executive functioning challenges, sensory processing differences, social communication demands, and anxiety, though these are distinct from specific learning disabilities in the clinical sense.
Should my autistic child be assessed for learning disabilities? I
f your child is struggling academically beyond what would be expected from their autism alone, a comprehensive assessment specifically looking for co-occurring learning disabilities is strongly recommended.
Does having autism mean my child will struggle at school?
Not necessarily, but autism does create specific challenges in educational settings that require appropriate accommodation and support to address effectively.
What is the difference between a learning disability and a learning difficulty?
In the US, learning disability is the clinical term for specific processing difficulties. In the UK, learning difficulty is used for similar conditions while learning disability refers to intellectual disability.
Final Thoughts
Is autism a learning disability? No, not in the US clinical framework. But that no answer should not be taken to mean that autism does not significantly affect learning, because it does, through a range of mechanisms that require real and specific educational accommodation.
And when learning disabilities co-occur with autism, which they do more often than most people realize, those learning disabilities deserve their own targeted identification and support alongside the broader autism support plan.
Getting this distinction right matters practically. It affects what assessments are requested, what support is put in place, and whether the autistic child or adult gets the full picture of what they need rather than a partial answer to an incomplete question.
References:
NHS. What is autism? [Internet]. Available from: https://www.nhs.uk/conditions/autism/what-is-autism/
Vallejo M. Is Autism a Learning Disability? [Internet]. Mental Health Center Kids; 2025 Jan 27. Available from: https://mentalhealthcenterkids.com/blogs/articles/is-autism-a-learning-disability
Congressional Research Service. The Individuals with Disabilities Education Act: A Comparison of State Eligibility Criteria [Internet]. Report R46566. 2020 Oct 12. Available from: https://www.congress.gov/crs-product/R46566
Knight C, Lowthian E, Jenks E, Jones C. The relationship between dyslexia, autism, and academic outcomes: longitudinal analysis of population-level education and health data. Oxf Rev Educ. 2025. Available from: https://doi.org/10.1080/03054985.2025.2590464
Academics West. A Parent's Guide to Qualifying Disabilities Under the IDEA [Internet]. 2026 Jan 30. Available from: https://academicswest.com/a-parents-guide-to-qualifying-disabilities-under-the-idea/

Is Autism Always Noticeable? What Most People Get Wrong
Is autism always noticeable? The short answer is no, and the gap between what most people expect autism to look like and what it actually looks like in many individuals is one of the most significant reasons autism goes unidentified for so long in so many people.
Is autism always noticeable is a question that matters for parents watching their child and wondering if what they are seeing is significant enough to pursue, and for adults who have spent years feeling different without ever having a name for why. In both cases, the assumption that autism is always visible and always obvious is one of the most persistent and most damaging myths in the public understanding of this condition.
This post unpacks what autism actually looks like across the full spectrum, why it is so often invisible, and what that invisibility costs the people living with it.
Table of Contents
Is Autism Always Noticeable? The Direct Answer
Where the Visible Autism Stereotype Comes From
What Invisible Autism Actually Looks Like
Why Autism Is Not Always Noticeable in Girls
The Role of Masking in Making Autism Invisible
Is Autism Always Noticeable at School
Is Autism Always Noticeable in Adults
The Cost of Invisible Autism
When Autism Becomes More Visible
FAQs
Final Thoughts
References
Is Autism Always Noticeable? The Direct Answer
Is autism always noticeable? No. Autism is not always noticeable, and in many cases it is actively invisible to the people closest to the autistic person, including parents, teachers, partners, and sometimes even the autistic person themselves.
The reason for this is not that the autism is less real or less impactful in these cases. It is that autism presents in an enormous range of ways, and many of those presentations do not match the image that most people carry in their heads when they think about what autism looks like. The child who is nonverbal, who rocks and flaps and does not make eye contact, is visible. The child who talks constantly about one specific topic, who manages socially by watching and copying peers, who holds it together at school and falls apart at home is far less visible. Both are autistic.
Is autism always noticeable depends entirely on which presentation you are looking at, which environment you are observing, and what you have been taught to look for.
Where the Visible Autism Stereotype Comes From
Understanding why people ask is autism always noticeable requires understanding where the stereotype of visible autism came from in the first place.
Early autism research, from the 1940s through to the 1990s, was conducted almost entirely on male children with significant support needs. The diagnostic criteria were developed from observations of this specific population, which meant the resulting picture of autism was dominated by the most visible and most impactful presentations. Autism became associated, in the public mind and in much of the clinical mind, with significant intellectual disability, absent or very limited speech, and highly visible repetitive behaviors.
As diagnostic criteria broadened and awareness grew, a much wider and more diverse population of autistic individuals began to be identified. Many of them looked almost nothing like the original stereotype. But the stereotype persisted in public consciousness long after the clinical picture had changed, and it continues to shape who gets identified, who gets believed, and who gets left without support.
What Invisible Autism Actually Looks Like
Is autism always noticeable in the people we might least expect? Absolutely not, and understanding what invisible autism looks like helps both parents and adults recognize it in themselves or their children.
Invisible autism often looks like:
A child who is highly verbal, academically capable, and appears to cope at school but who comes home and falls apart completely
A child who watches peers carefully and copies their behavior with enough success that the underlying difficulty is not visible from the outside
An adult who has built a functional life but who finds it exhausting in ways they cannot fully explain to anyone around them
Someone who is described as quirky, intense, or a bit different but who has never been flagged as autistic because they manage well enough in structured environments
A person whose sensory sensitivities, rigid routines, and social exhaustion are attributed to personality traits, anxiety, or simply being an introvert
None of these presentations are unusual. They are in fact among the most common ways autism presents across the population once you move beyond the most visible end of the spectrum.
Why Autism Is Not Always Noticeable in Girls
Is autism always noticeable in girls? Even less so than in boys, and this is one of the most significant and best-documented sources of missed diagnosis in the autism community.
Girls with autism are significantly more likely to mask their autistic traits than boys. They observe social behavior carefully, imitate it, and use their social awareness to compensate for the genuine social communication differences underneath. The result is a presentation that can look like shyness, social anxiety, or simply being quiet rather than autism.
Research found that autistic females showed significantly greater camouflaging of autistic traits than autistic males, with the degree of camouflaging contributing directly to delayed diagnosis and increased mental health burden.
Is autism always noticeable in the girls sitting quietly in the back of classrooms, managing socially with enormous effort, and coming home completely depleted? Almost never. And the cost of that invisibility is measured in years of missed support, compounding anxiety, and a quiet sense of being wrong about themselves that most of these girls carry into adulthood before they ever receive a diagnosis.
This is one of the conversations that comes up regularly on the On the Spectrum podcast with Sonia Chand, where real, honest discussions about the autism journey, including who gets seen and who does not, happen in a way that is genuinely useful for families and individuals trying to navigate this.
Listen to the On the Spectrum podcast here and find the conversations that help you see autism more clearly, in all the forms it actually takes.
The Role of Masking in Making Autism Invisible
Is autism always noticeable when the autistic person is actively working to make it invisible? This is the reality for a significant proportion of autistic people, and it is called masking.
Masking is the conscious or semi-conscious suppression of autistic traits in order to appear more neurotypical. It involves forcing eye contact that feels uncomfortable, using rehearsed scripts for social interactions, suppressing stimming in public, and performing calm when internally dysregulated. For many autistic people, masking becomes so automatic over time that they themselves are not fully aware they are doing it.
Masking is directly relevant to the question of is autism always noticeable because it is one of the primary mechanisms through which autism becomes invisible, both to observers and sometimes to the autistic person themselves.
Research identified masking as a significant factor in delayed autism diagnosis and found it was associated with substantially higher rates of depression, anxiety, and suicidal ideation in autistic individuals, particularly women.
The cost of masking is high and it is real, and understanding it is one of the most important parts of understanding why autism is not always noticeable.
If you are an autistic adult who has spent years masking and is now starting to understand what that has cost you, Dropped in a Maze by Sonia Chand speaks directly to that experience. It is the honest account of navigating an autism journey without a clear map, and it captures the exhaustion of going unseen in a way that very few books manage.
Get your copy of Dropped in a Maze here and find the words for an experience you may have been carrying alone for a very long time.
Is Autism Always Noticeable at School
Is autism always noticeable in a school environment? For many autistic children, school is precisely the place where autism is least visible, because school provides the structured, predictable environment that autistic children often manage best.
Many autistic children hold themselves together through the school day using enormous amounts of cognitive and emotional energy. They follow the routine, they stay in their seat, they do their work, and they appear to be managing. Teachers who do not know what to look for, and who are working with large classes under significant pressure, may see only the surface level of functioning rather than the effort underneath it.
Is autism always noticeable at home? Much more so, because home is where the mask comes off. The child who appeared fine at school is explosive, exhausted, or completely shut down at home. This pattern, doing well at school and falling apart at home, is one of the most consistent signs of invisible autism in children and one that is frequently misunderstood by both parents and schools.
For parents who are navigating this exact pattern and trying to figure out whether what they are seeing warrants a formal evaluation, the post on how to test for autism covers the entire assessment process from first concern through to diagnosis.
Is Autism Always Noticeable in Adults
Is autism always noticeable in adults? Even less so than in children, for several compounding reasons.
By adulthood, many autistic people have spent decades building compensatory strategies for the things that do not come naturally. They have developed scripts for social situations, careers that play to their strengths, and routines that reduce the daily demand on their nervous system. The autism is still there, shaping every aspect of how they experience the world, but the compensatory scaffolding around it can make it almost entirely invisible to people who do not know what they are looking for.
Many adults discover they are autistic for the first time only after a child receives a diagnosis and the parent recognizes their own childhood in the child's traits. Others get there after years of therapy for anxiety, depression, or burnout that never quite got to the root of what was actually driving those experiences.
Is autism always noticeable when an autistic adult walks into a room? Almost never. And for the adult who has spent a lifetime not understanding themselves, that invisibility has a cost that is real and deep and deserves real and skilled support.
Coaching with Sonia offers exactly that, personalised, neurodivergent-affirming support for adults who are finally putting the pieces together and building a life that works for their actual brain rather than the neurotypical one they have been performing for decades.
Book a coaching session with Sonia here and start getting support that finally understands how you are actually wired.
The Cost of Invisible Autism
Is autism always noticeable is ultimately a question about who gets seen, and the answer has direct consequences for who gets help.
When autism is not noticeable, it does not get identified. When it does not get identified, the autistic person does not receive the understanding, accommodation, and support they need. The mental health consequences of that gap are significant and well-documented: higher rates of anxiety, depression, burnout, and suicidal ideation in autistic individuals who are identified late or not at all.
The cost of invisible autism is also relational. Years of not understanding why social situations feel so hard, why relationships struggle in ways that are difficult to explain, and why the exhaustion never seems to lift takes a toll that persists even after a diagnosis eventually arrives.
For a deeper understanding of what happens when autism goes without the right support, the post on if autism is left untreated covers the research and the real-world consequences in full.
When Autism Becomes More Visible
Is autism always noticeable even in people who usually mask effectively? There are specific circumstances where autism becomes more visible even in people who have compensated effectively for years.
These include periods of significant stress or change, major life transitions such as starting university or a new job, physical illness that depletes the energy available for masking, periods of autistic burnout, and environments that are significantly more sensory or socially demanding than usual.
Understanding this helps explain why autism sometimes seems to appear suddenly in people who previously appeared to be managing well. The autism was always there. The circumstances simply changed enough that the usual compensatory strategies could no longer hold.
FAQs
Is autism always noticeable?
No. Many autistic people, particularly women, late-diagnosed adults, and those who mask effectively, present in ways that are not visibly recognizable as autism.
Can someone be autistic and appear completely typical?
Yes. Effective masking, compensation strategies, and structured environments can make autism essentially invisible to outside observers.
Can autism become more visible over time?
Yes. During periods of significant stress, burnout, or major life transitions, autism often becomes more visible even in people who have compensated effectively for years.
Is invisible autism less severe than visible autism?
No. The internal experience and impact of invisible autism can be just as significant as more visible presentations. Invisible autism often involves intense masking that has significant mental health consequences.
Can a doctor miss autism because it is not noticeable?
Yes. This happens regularly, particularly for women, adults, and individuals who present outside the most visible stereotype of autism.
What should I do if I suspect autism but it is not obviously noticeable?
Document specific behaviors across multiple settings, trust your observations, and request a formal evaluation from a clinician with specific experience in the less visible presentations of autism.
Final Thoughts
Is autism always noticeable? No. And that simple answer carries enormous implications for the millions of autistic people who have gone unidentified, unsupported, and unseen because the people around them were looking for something that did not match what they actually were.
Autism is visible when we know what to look for. It is visible in the child who holds it together all day and falls apart at home. It is visible in the adult who is exhausted in ways they cannot fully explain. It is visible in the years of anxiety, depression, and burnout that accumulate when the right framework and the right support never arrive.
Learning to see autism in all its forms, not just the most obvious ones, is one of the most important things we can do for the autistic people in our lives and for the autistic people who do not yet know that is what they are.
References:
Augie. The diagnosis story [Internet]. Autistic Pride Day; 2025 Jan 14. Available from: https://autisticprideday.org/diagnosis-history/
Wood-Downie H, Wong B, Kovshoff H, Mandy W, Hull L, Hadwin JA. Sex/Gender Differences in Camouflaging in Children and Adolescents with Autism. J Autism Dev Disord. 2021;51(4):1353-1364. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7985051/
Conde-Pumpido-Zubizarreta S, Cruz S, Pozo-Rodríguez M, Suárez-Rama JJ, Díaz-Hernández A, Carracedo A, Tubío-Fungueiriño M, Fernández-Prieto M. The association between autism, camouflaging and anxiety with suicidal ideation in women. Front Psychol. 2026;16:1685845. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12879100/
UNICEF. Autism symptoms: Common signs of ASD in children [Internet]. 2025 Apr 2. Available from: https://www.unicef.org/eca/stories/autism-symptoms-common-signs-asd-children
Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). What are the symptoms of autism? [Internet]. Last reviewed 2025 Dec 23. Available from: https://www.nichd.nih.gov/health/topics/autism/conditioninfo/symptoms

If Autism Is Left Untreated: What Actually Happens and Why It Matters
If autism is left untreated is one of the most searched questions about autism, and it carries a weight that most other search queries do not. Behind it is usually a parent who is scared, or an adult who is starting to wonder whether years of struggling without a diagnosis has quietly cost them more than they realized.
The honest answer to what happens if autism is left untreated is not simple, because autism is not a single condition with a single trajectory. What happens depends enormously on the individual, their specific profile, their environment, and what kind of support was or was not available to them. But the research is clear enough on several key points that it is worth addressing directly and honestly, without either minimizing the real consequences or catastrophizing in ways that help nobody.
This post covers what the research actually says about what happens if autism is left untreated, what untreated really means in this context, and what genuinely changes when the right support finally arrives.
Table of Contents
What Does Untreated Actually Mean in Autism
If Autism Is Left Untreated: Mental Health Consequences
If Autism Is Left Untreated: Communication and Social Development
If Autism Is Left Untreated: Education and Employment
If Autism Is Left Untreated: Relationships and Isolation
If Autism Is Left Untreated: Physical Health
The Difference the Right Support Makes
It Is Never Too Late
FAQs
Final Thoughts
What Does Untreated Actually Mean in Autism
Before going further it is worth being clear about what untreated actually means in the context of autism, because the word treatment carries different implications here than it does in the context of a disease or infection.
Autism is not a disease. It cannot be cured and it does not need to be. When people ask what happens if autism is left untreated, what they are really asking is: what happens when an autistic person goes without the understanding, accommodation, support, and tools they need to navigate a world that was not designed for their neurology.
Untreated in autism means unidentified, unsupported, and unaccommodated. It means a child growing up without anyone around them understanding why things are hard, without the right educational support, without the communication tools they need, and without the framework to make sense of their own experience. It means an adult spending decades wondering why they are different, why relationships are so hard, and why they are so exhausted by things that seem effortless for everyone else.
When framed that way, the question of what happens if autism is left untreated becomes both clearer and more urgent.
If Autism Is Left Untreated: Mental Health Consequences
The most consistently documented consequence of autism being left untreated is significant mental health impact.
Research published in the journal Autism in Research found that autistic individuals who are undiagnosed or who receive a late diagnosis report significantly higher rates of anxiety and depression than those identified and supported earlier..
This is not a coincidence. If autism is left untreated, the autistic person spends years, sometimes decades, trying to function in an environment that does not accommodate them, masking their natural responses, absorbing repeated messages that they are too much, too sensitive, too rigid, or simply not trying hard enough. That accumulated experience has a real and measurable cost.
Anxiety and depression in unidentified autism are not separate conditions that happen to occur alongside autism. They are frequently the direct result of what happens when autism is left untreated and the gap between what the autistic person needs and what they receive goes unaddressed year after year.
If Autism Is Left Untreated: Communication and Social Development
For children in particular, if autism is left untreated during the critical early developmental window, communication and social development are among the most significantly affected areas.
The brain is most neuroplastic in the earliest years of life. When autism is identified early and the right communication support is put in place during that window, children develop stronger functional communication skills than they would develop without it. When autism is left untreated during that same window, the gaps between the autistic child and their neurotypical peers in both communication and social skill development tend to widen rather than close on their own.
This does not mean that communication development stops or that social skills cannot be built later. Many autistic individuals make significant gains in both areas throughout childhood, adolescence, and adulthood. But the research is consistent that earlier support produces better outcomes, and the absence of early support leaves gaps that take more effort to address later.
For children who are nonverbal or minimally verbal, if autism is left untreated the consequences for communication are particularly significant because the window for establishing an alternative communication channel, such as AAC, is also most effective in the early years.
The post on early autism detection covers in detail why early identification and early support make such a measurable difference, and is worth reading alongside this one.
If Autism Is Left Untreated: Education and Employment
If autism is left untreated, the consequences ripple through education and into adult employment in ways that compound over time.
In school, an autistic child without identification or support is typically expected to meet the same academic and behavioral standards as neurotypical peers, without the accommodations that would allow them to actually demonstrate what they know. Sensory overload goes unaddressed. Executive functioning difficulties go unsupported. Social misunderstandings accumulate and affect both peer relationships and teacher relationships. Many autistic children without identification are labeled as lazy, difficult, disruptive, or underachieving, when the reality is that they are working significantly harder than anyone around them realizes just to get through the day.
In employment, the picture for adults if autism is left untreated is similarly challenging. Research from Drexel University's Autism Institute found that autistic adults have among the lowest employment rates of any disability group, with many struggling to maintain employment not because of lack of ability but because of the absence of accommodations, the demands of masking, and the social complexity of workplace environments that were not designed for autistic brains.
Dropped in a Maze by Sonia Chand is one of the most honest accounts of what it looks like to navigate the autism journey without a clear map, and it is exactly the kind of reading that helps families and autistic individuals understand not just what support is needed but how to find their way through a system that does not always make it easy.
Get your copy of Dropped in a Maze here
If Autism Is Left Untreated: Relationships and Isolation
If autism is left untreated, relationships are one of the areas where the impact accumulates most quietly and most painfully.
Without a framework for understanding their own social communication differences, autistic people often experience repeated relationship failures that they cannot explain or prevent. Friendships that start well and then inexplicably fall apart. Romantic relationships that struggle under the weight of unmet communication needs. Family relationships strained by years of being misunderstood. The absence of a diagnosis means the absence of a shared language for understanding what is actually happening in these relationships and what would genuinely help.
Social isolation is one of the most consistent findings in research on untreated autism across the lifespan. And social isolation, in turn, significantly worsens the mental health consequences already described above.
If you are navigating these relationship and communication challenges and looking for practical, personalised support built around your actual neurology, coaching with Sonia is exactly the kind of help that makes a real difference.
Book a coaching session with Sonia here and start building the communication tools and social confidence that change how relationships actually feel.
If Autism Is Left Untreated: Physical Health
Physical health is an often overlooked area of what happens if autism is left untreated, but the research here is worth taking seriously.
Autistic individuals have higher rates of several physical health conditions including gastrointestinal disorders, sleep disorders, and epilepsy. When autism is left untreated and unidentified, these co-occurring conditions are frequently also missed, misattributed, or managed inadequately because the underlying autism context that would help clinicians understand them is not recognized.
Sleep disorders in particular have a significant downstream impact on every other area of functioning including mental health, cognitive performance, emotional regulation, and daily functioning. When autism is left untreated, sleep issues are often attributed to behavioral causes rather than the neurological differences driving them, leading to interventions that do not address the actual problem.
Research published in the journal Sleep Medicine Reviews has found that sleep disturbances affect between 40 and 80 percent of autistic individuals and that addressing them has significant positive effects on daytime functioning, behavior, and quality of life.

The Difference the Right Support Makes
Understanding what happens if autism is left untreated is most useful when paired with an equally clear picture of what changes when the right support is finally in place.
When autism is identified and supported appropriately, anxiety decreases because the autistic person finally has a framework for understanding their own experience. Communication improves because the right tools and strategies are available. Relationships become easier to navigate because there is shared language for what is actually happening. Employment becomes more sustainable because accommodations can be requested and implemented. And the years of accumulated self-blame, shame, and confusion begin to give way to something more accurate and more compassionate.
The On the Spectrum podcast with Sonia Chand covers exactly these kinds of real, honest conversations about what the journey from untreated to genuinely supported looks like, with guests who have navigated it themselves and with the kind of practical insight that makes a real difference.
Listen to the On the Spectrum podcast here and find the conversations that make the journey feel less impossible.
The right support does not undo the years that passed without it. But it can genuinely change what the years ahead look like, and that is worth everything.
It Is Never Too Late
One of the most important things to say about if autism is left untreated is that the damage is not permanent and it is never too late for the right support to make a genuine difference.
Adults who are diagnosed later in life consistently report that the diagnosis, even when it comes decades after it should have, changes things. The framework it provides for understanding a lifetime of experiences has real and lasting value. The support it opens access to, whether that is workplace accommodations, appropriate therapy, or coaching built around actual autistic neurology, makes a measurable difference to quality of life regardless of when it arrives.
For autistic adults who are recognising themselves in this post and wondering where to start, coaching with Sonia offers exactly the kind of personalised, neurodivergent-affirming support that meets you exactly where you are right now.
FAQs
What happens if autism is left untreated?
Without identification and support, autistic individuals face significantly higher rates of anxiety, depression, social isolation, educational underachievement, and employment difficulties.
Can autism get worse if left untreated?
Autism itself does not worsen, but the secondary consequences including mental health, relationships, and life opportunities are significantly worse without appropriate support.
Is it too late to get support for autism as an adult?
No. Support at any age makes a meaningful difference to quality of life, and adult diagnosis opens access to accommodations and understanding that were previously unavailable.
What is the most important thing to do if autism has gone unidentified?
Pursue formal assessment, access appropriate support as soon as possible, and connect with community. The clarity that comes from identification, even late, changes things meaningfully.
Can the effects of untreated autism be reversed?
Many of the secondary consequences can be significantly improved with the right support. The earlier the support arrives the better, but meaningful improvement is possible at any age.
Final Thoughts
If autism is left untreated, the consequences are real, they are documented, and they compound over time. But they are not inevitable, and they are not permanent.
The difference between an autistic person who goes without support and one who receives the right support at the right time is not a difference in the autism itself. It is a difference in whether the world around them made room for who they actually are.
That room can be made at any point. And making it, however late it comes, matters.
References:
Autism Research Institute. Treating Sleep Disorders [Internet]. Last updated September 2024. https://autism.org/treating-sleep-disorders/
Belenguer LM, Cabrera TDLC, Arboledas GP. Sleep Characteristics in Children and Adolescents With Autism Spectrum Disorder. J Sleep Med. 2025 Aug;22(2):49-62.https://www.e-jsm.org/journal/view.php?number=415
Roux AM, Shattuck PT, Rast JE, Rava JA, Anderson KA. National Autism Indicators Report: Transition into Young Adulthood. Philadelphia, PA: Life Course Outcomes Research Program, A.J. Drexel Autism Institute, Drexel University; 2015.https://drexel.edu/~/media/Files/autismoutcomes/publications/LCO%20Fact%20Sheet%20Employment.ashx

What Is Level 3 Autism? A Complete Guide for Parents and Families
What is level 3 autism is a question that often comes with real weight behind it, because Level 3 sits at the most complex end of the autism spectrum and the answer touches on some of the biggest, most life-shaping questions a parent or family member can ask. If you are here because your child, sibling, or loved one has just received this designation, or because you suspect it might apply, you deserve a clear, honest, and complete answer.
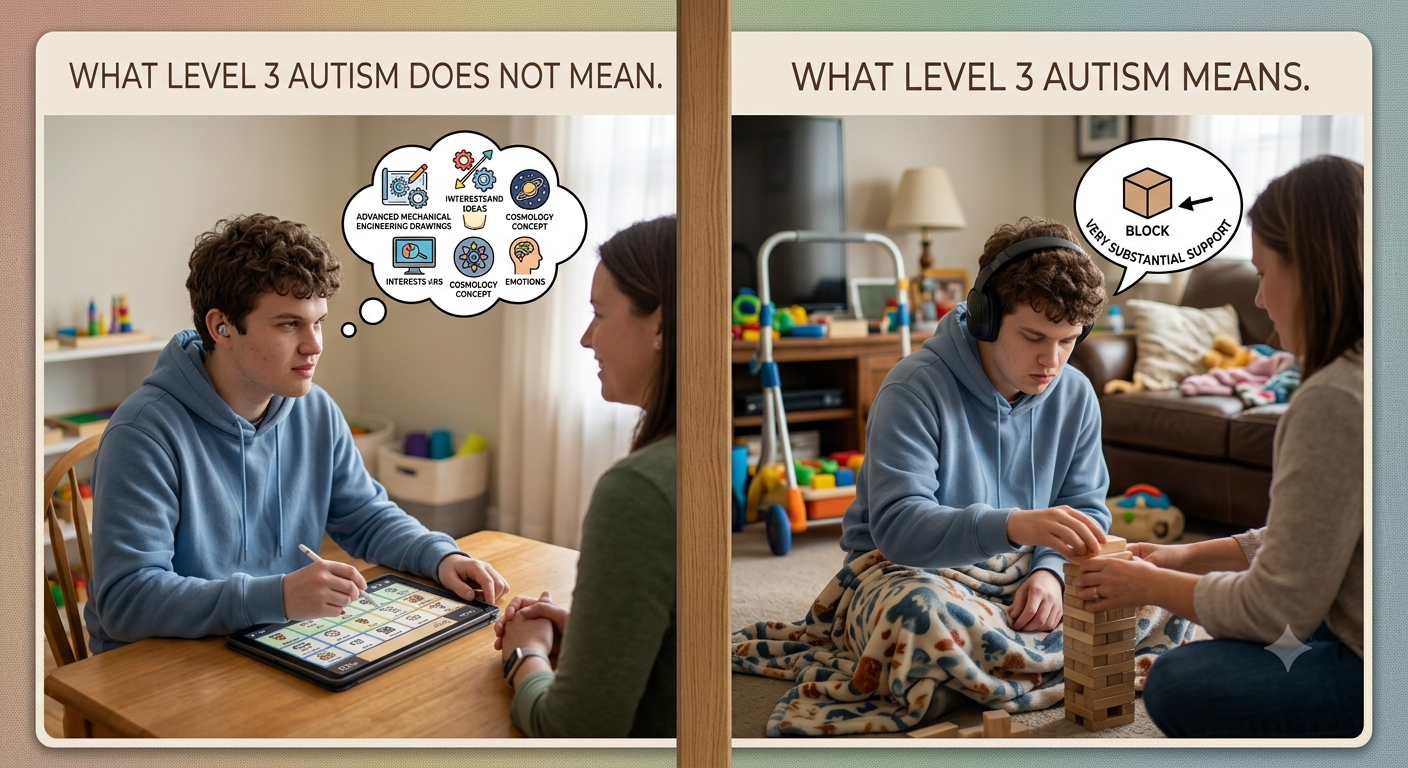
What is level 3 autism in the simplest terms is the official DSM-5 designation for autistic individuals who require very substantial support. It is the highest of the three official autism support levels, describing the most significant and pervasive impact on social communication and behavior that the diagnostic system currently recognizes.
This post answers what is level 3 autism in full, what it actually looks like in daily life, how it compares to Level 1 and Level 2, and what genuinely helps families and individuals navigating this end of the spectrum.
Table of Contents
What Is Level 3 Autism?
Where Level 3 Autism Sits on the Spectrum
Signs and Characteristics of Level 3 Autism
Communication and Level 3 Autism
Level 3 Autism vs Level 2 Autism
Level 3 Autism vs Level 1 Autism
How Level 3 Autism Is Diagnosed
What Daily Life Looks Like With Level 3 Autism
What Level 3 Autism Does Not Mean
What Support Actually Looks Like for Level 3 Autism
Final Thoughts
What Is Level 3 Autism?
What is level 3 autism according to the DSM-5? It is described as requiring very substantial support, the most significant of the three official levels. The manual defines it as severe deficits in verbal and nonverbal social communication skills that cause severe impairments in functioning, along with restricted, repetitive behaviors that markedly interfere with functioning across all areas of life.
What is level 3 autism in practical terms is a profile where support is not occasional or supplementary. It is constant, pervasive, and necessary across nearly every domain of daily living, including communication, self-care, safety, and community participation.
What is level 3 autism not is a measure of a person's worth, potential for connection, or capacity for a meaningful life. It is a description of current support needs as assessed in a specific clinical evaluation. It tells you how much support someone needs right now. It does not tell you who they are or what they are capable of experiencing, learning, or feeling.
Where Level 3 Autism Sits on the Spectrum
Understanding what is level 3 autism means seeing it clearly against the other two levels.
Level 1 autism involves support needs that a person can often manage with personal effort, without support being constantly present. Level 2 autism involves support needs that remain apparent and necessary even when support is actively provided, but that still allow for meaningful independence in some areas of life.
Level 3 autism involves support needs that are severe and pervasive enough that they affect functioning across nearly all domains, even when substantial, consistent support is already in place. What is level 3 autism, set against this scale, is the profile with the most significant and far-reaching impact on daily functioning that the current diagnostic system describes.
Signs and Characteristics of Level 3 Autism
What is level 3 autism actually looks like in practice involves a combination of communication, behavioral, and sensory characteristics that are significant and consistent across settings.
Social communication characteristics:
Very limited initiation of social interaction, often appearing to show minimal interest in social engagement as it is typically understood
Minimal response to social overtures from others, including from familiar caregivers
Severe difficulties with both verbal and nonverbal communication
Communication, when present, is often limited to expressing immediate needs rather than broader social or emotional exchange
Restricted and repetitive behavior characteristics:
Repetitive behaviors that are intense, frequent, and significantly interfere with functioning across multiple settings
Extreme distress in response to changes in routine or environment
Restricted interests or behaviors that dominate a significant portion of daily activity
Difficulty redirecting attention away from repetitive patterns even with active support
Sensory characteristics:
Significant sensory sensitivities that affect what environments and activities are tolerable
Strong reactions to sensory input that others may not perceive at all
Sensory needs that require ongoing, active accommodation rather than occasional adjustment
Daily functioning characteristics:
Significant support needs across most or all areas of daily living, including self-care tasks such as dressing, hygiene, and eating
Safety awareness that requires ongoing supervision and support
Higher rates of co-occurring conditions including epilepsy, gastrointestinal issues, and sleep disorders

Communication and Level 3 Autism
Communication is one of the most significant areas affected by what is level 3 autism, and it is also one of the areas where the right support makes the most measurable difference.
Many individuals with Level 3 autism have little to no functional spoken language. This does not mean they have nothing to communicate. It means spoken language is not a reliable channel for them to express their needs, preferences, and experiences.
Augmentative and Alternative Communication, known as AAC, is often transformative for individuals with Level 3 autism. This ranges from simple picture exchange systems to sophisticated speech generating devices, and finding the right communication channel is consistently one of the highest impact interventions available.
It is worth being direct about something important here: a person with Level 3 autism who cannot speak is not a person without thoughts, preferences, or an inner life. They are a person whose primary communication channel has not yet been found or fully supported. The research on AAC consistently shows that many nonverbal autistic individuals have far more to communicate than their spoken output suggests once the right tool is in place.
Level 3 Autism vs Level 2 Autism
Comparing what is level 3 autism against what is level 2 autism helps clarify exactly where the line sits between them.
Level 2 autism involves social communication deficits that remain apparent even with support, but the person often retains functional spoken language and can manage some independence in daily living with consistent structural support. Level 3 autism involves more severe deficits that cause significant impairment even with very substantial support actively in place, and functional spoken language is frequently absent or extremely limited.
Repetitive behaviors at Level 2 interfere with functioning across multiple settings but are often manageable with redirection and support. At Level 3, these behaviors are more intense and markedly interfere with functioning even when active support is provided.
Daily living independence is more achievable at Level 2 in many domains. At Level 3, support needs typically extend across nearly all areas of daily living, including self-care and safety.
For a complete look at what Level 2 autism involves specifically, the post on what is level 2 autism covers that middle point on the spectrum in full detail.

Level 3 Autism vs Level 1 Autism
Comparing what is level 3 autism against what is level 1 autism shows the full range the diagnostic system is trying to capture under a single spectrum.
Level 1 autism, sometimes informally called high functioning autism, involves support needs that a person can often manage independently, with social communication challenges that are noticeable but generally compatible with functioning in most everyday settings without support being constantly present.
Level 3 autism sits at the opposite end, with support needs that are constant, pervasive, and necessary across nearly every area of daily life, even when substantial support is already in place. Aside these, Dropped in a Maze provides a clear picture on how to navigate autism.
The distance between these two ends of the spectrum is part of why autism is described as a spectrum rather than a single condition with one presentation. Two people can both carry an autism diagnosis and have profiles, support needs, and daily experiences that look almost entirely different from one another. For a closer look at the other end of this range, the post on what is level 1 autism covers that presentation in depth.
How Level 3 Autism Is Diagnosed
What is level 3 autism in terms of the actual diagnostic process follows the same general framework used across the spectrum, though the evaluation often happens earlier in life because the signs tend to be more pronounced and visible from a younger age.
A comprehensive evaluation typically includes a detailed developmental history from parents or caregivers, direct behavioral observation using tools such as the ADOS-2, cognitive and language assessment adapted for the individual's communication level, and input from other professionals including speech therapists and occupational therapists who know the child or adult well.
For a full walkthrough of the entire testing and diagnostic process from first screening through to full evaluation, the post on how to test for autism covers exactly what families can expect at every stage.
What Daily Life Looks Like With Level 3 Autism
What is level 3 autism in lived, daily terms varies depending on the individual, but it generally involves a level of structure, support, and consistency that shapes most of the day.
Daily routines are often highly structured because predictability significantly reduces distress and supports functioning. Communication happens through whatever channel works best for that individual, whether AAC devices, gestures, behavior, or limited functional speech. Sensory environments are actively managed, with lighting, sound, and textures considered and adjusted wherever possible. Safety supervision is ongoing rather than occasional, particularly for individuals who may not reliably understand environmental risks.
None of this means daily life with Level 3 autism is without joy, connection, or genuine quality of life. Many individuals with Level 3 autism experience real happiness, form meaningful bonds with the people who know how to connect with them, and respond strongly to music, movement, sensory play, and the presence of people who make them feel safe.
Level 3 Autism
What Level 3 Autism Does Not Mean
This matters as much as anything else in this post, because some of the most harmful assumptions about Level 3 autism come from what people wrongly believe the label implies.
What is level 3 autism does not mean the person has no inner life, no preferences, and no capacity for growth. It does not mean communication is impossible, only that spoken language may not be the right channel. It does not mean the person cannot learn or make meaningful progress with the right support over time. It does not mean their life has less value than the life of someone with Level 1 autism. It does not mean families should lower their hopes for connection and quality of life.
The person is always there. What changes with the right support is how clearly the people around them can see and understand who that person actually is.
What Support Actually Looks Like for Level 3 Autism
Support for what is level 3 autism needs to be comprehensive, consistent, and genuinely tailored to the individual, drawing on several areas working together.
Communication support through AAC evaluation and implementation is consistently one of the highest impact interventions. Educational support under an IEP that addresses communication, behavioral, and daily living goals specifically is essential. Behavioral support that is positive and function-based, focused on understanding what a behavior is communicating rather than simply suppressing it, produces far better outcomes than punitive approaches. Medical management addressing the higher rates of epilepsy, gastrointestinal issues, and sleep disorders associated with Level 3 autism is an important and often overlooked part of comprehensive care.
Ready to navigate this with support? Sonia, a licensed psychotherapist provides Adult Coaching Services
Final Thoughts
What is level 3 autism is, at its core, a description of the most significant and pervasive support needs the current diagnostic system recognizes. It is not a description of a person's worth, their capacity for connection, or the ceiling on their growth.
The families and individuals navigating Level 3 autism deserve fully resourced, genuinely informed, deeply compassionate support, and that support, when it arrives in the right form at the right time, makes a real and lasting difference to quality of life for everyone involved.
References:
Iacono T, Trembath D, Erickson S. The role of augmentative and alternative communication for children with autism: current status and future trends. Neuropsychiatr Dis Treat. 2016;12:2349-2361. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5036660/
Lin W, Chan YH, Kiing JSH, Lim TSH, Chong SC, Kang YQ, Aishworiya R, Mulay KV, Tan MY. Restricted and repetitive behaviors and association with cognition and adaptive functioning in children with autism spectrum disorder in Singapore. Front Psychiatry. 2023;14:1249071. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10687550/
American Speech-Language-Hearing Association. Augmentative and Alternative Communication in Early Intervention [Internet]. Available from: https://www.asha.org/practice/early-intervention-provider-support/augmentative-and-alternative-communication-in-early-intervention/
Maddox BB, Brodkin ES, Calkins ME, Shea K, Mullan K, Hostager J, Mandell DS, Miller JS. The accuracy of the ADOS-2 in identifying autism among adults with complex psychiatric conditions. J Autism Dev Disord. 2017;47(9):2703-2709. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5813679/

Is Autism an Intellectual Disability? What Parents Need to Know
Is autism an intellectual disability is one of the most commonly searched questions about autism and one of the most frequently misunderstood. Parents hear the term intellectual disability in the same conversation as their child's autism diagnosis and immediately wonder whether the two are the same thing, whether one causes the other, and what it means for their child's future.
Is autism an intellectual disability deserves a clear, direct answer because the confusion between the two has real consequences for how autistic children are seen, how they are supported, and what opportunities they are given access to.
This post answers the question is autism an intellectual disability honestly and completely, explains what both terms actually mean, looks at where they overlap and where they do not, and gives parents the practical information they need to advocate effectively for their child.
Table of Contents
Is Autism an Intellectual Disability?
What Is Autism?
What Is an Intellectual Disability?
Where Autism and Intellectual Disability Overlap
Where Autism and Intellectual Disability Differ
How Common Is Intellectual Disability in Autism?
Why Is Autism So Often Confused With Intellectual Disability?
The Problem With Assuming Intellectual Disability in Autism
How This Connects to Profound Autism
The Role of Coaching and Support
FAQs
Final Thoughts
Is Autism an Intellectual Disability?
Is autism an intellectual disability? No. Autism and intellectual disability are two separate conditions. They can co-occur in the same person but they are not the same thing and one does not cause the other.
Autism is a neurodevelopmental condition characterized by differences in social communication, sensory processing, and restricted or repetitive behaviors. Intellectual disability is a separate condition characterized by significant limitations in both intellectual functioning and adaptive behavior that originate before the age of 18.
Is autism an intellectual disability in the sense that autism always involves limited intellectual functioning? No. The majority of autistic people do not have an intellectual disability. Many autistic people have average, above average, or exceptional intellectual abilities.
Is autism an intellectual disability in the sense that intellectual disability and autism share some features? Yes, in limited ways. Both are neurodevelopmental conditions. Both are present from early childhood. And in some autistic individuals, both occur together. But having one does not mean having the other.
The confusion between the two is understandable given how frequently they are discussed together and how significantly intellectual disability affects the autism presentation when it is present. But the confusion has real costs when it leads to autistic children being underestimated, placed in inappropriate settings, or denied opportunities because someone assumed their autism meant intellectual disability.
What Is Autism?
Before going deeper into the question of is autism an intellectual disability, it helps to be clear about what each term actually means.
Autism, formally known as Autism Spectrum Disorder or ASD, is a neurodevelopmental condition that affects how a person communicates, processes information, experiences sensory input, and relates to others. It is present from birth and it is lifelong.
The core features of autism are:
Differences in social communication and social interaction across multiple contexts
Restricted, repetitive patterns of behavior, interests, or activities
Sensory processing differences that affect how the person experiences and responds to sensory input
Autism presents very differently across individuals. Some autistic people are nonverbal and require significant support across all areas of daily life. Others are highly verbal, academically capable, and manage many daily tasks independently. The spectrum is genuinely wide and the variability within it is enormous.
What autism does not inherently involve is limited intellectual functioning. Intellectual ability in autism ranges across the full spectrum from significant intellectual disability to exceptional intellectual gifts. Autism describes a neurological profile. It does not specify intelligence.
For a comprehensive understanding of what autism is at a neurological level and why the brain works differently in autistic people, the post on is autism a neurological disorder covers neuroscience in depth.
Dropped in a Maze, one of the bestselling books on Autism
What Is an Intellectual Disability?
Intellectual disability, formerly known as mental retardation in older clinical literature, is defined by three criteria that must all be present:
Significant limitations in intellectual functioning: An IQ score approximately two standard deviations below the mean, which typically means an IQ below 70, along with clinical judgment confirming significant cognitive limitations.
Significant limitations in adaptive behavior: Difficulty with the practical skills needed for everyday life including conceptual skills such as language and literacy, social skills such as interpersonal relationships and following rules, and practical skills such as personal care, managing money, and managing routines.
Onset during the developmental period: The limitations must be present before the age of 18, distinguishing intellectual disability from acquired cognitive impairments that develop in adulthood through injury or disease.
Intellectual disability ranges in severity from mild to moderate to severe to profound. The majority of people with intellectual disability, around 85 percent, have mild intellectual disability and can develop significant life skills with appropriate support.
Is autism an intellectual disability by this definition? No. Autism does not inherently involve significant limitations in intellectual functioning. An autistic person with an IQ of 120 has no intellectual disability. An autistic person with an IQ of 45 may have both autism and intellectual disability as co-occurring conditions.
Where Autism and Intellectual Disability Overlap
While is autism an intellectual disability has a clear no answer, autism and intellectual disability do overlap in some important ways that are worth understanding.
They can co-occur: Autism and intellectual disability are separate conditions but they frequently occur together in the same individual. Research suggests that somewhere between 30 and 40 percent of autistic people also have an intellectual disability. This co-occurrence is real and significant and it shapes the support needs and life experiences of those individuals in profound ways.
They are both neurodevelopmental: Both autism and intellectual disability are classified as neurodevelopmental conditions in the DSM-5. Both originate in differences in brain development during the prenatal and early postnatal period. Both are present from birth even when not identified until later.
They both affect learning: Both autism and intellectual disability can affect how a person learns, though they affect learning differently. Autism affects learning through differences in social communication, sensory processing, and information processing style. Intellectual disability affects learning through limitations in cognitive processing speed, working memory, and abstract reasoning.
They are both lifelong: Neither autism nor intellectual disability is something a person grows out of. Both are permanent aspects of the person's neurology. Support needs may change over time but the underlying conditions remain.
They both qualify for educational support: Both autism and intellectual disability qualify children for Individualized Education Programs under IDEA and for special education services. When they co-occur, the educational planning needs to address both conditions.
Where Autism and Intellectual Disability Differ
Understanding where autism and intellectual disability differ is just as important as understanding where they overlap, particularly when answering the question of is autism an intellectual disability.
Intellectual functioning: The most fundamental difference is that autism does not inherently involve limited intellectual functioning while intellectual disability does by definition. Autistic people can have IQs at any point on the full range of human cognitive ability.
Social communication: Autism specifically involves differences in social communication that are not explained by intellectual disability alone. An autistic person without intellectual disability has specific social communication differences that a person with intellectual disability of the same cognitive level would not necessarily have.
Sensory processing: Sensory processing differences are a core feature of autism and are not a defining feature of intellectual disability. Many autistic people have significant sensory sensitivities that profoundly affect their daily functioning in ways that are distinct from the challenges of intellectual disability.
Restricted and repetitive behaviors: The restricted and repetitive behaviors that characterize autism, including special interests, insistence on sameness, and repetitive movements, are not defining features of intellectual disability.
Cause: The genetic and neurological underpinnings of autism and intellectual disability differ significantly even though both involve differences in brain development. They represent distinct developmental pathways that happen to co-occur more frequently than chance would predict.
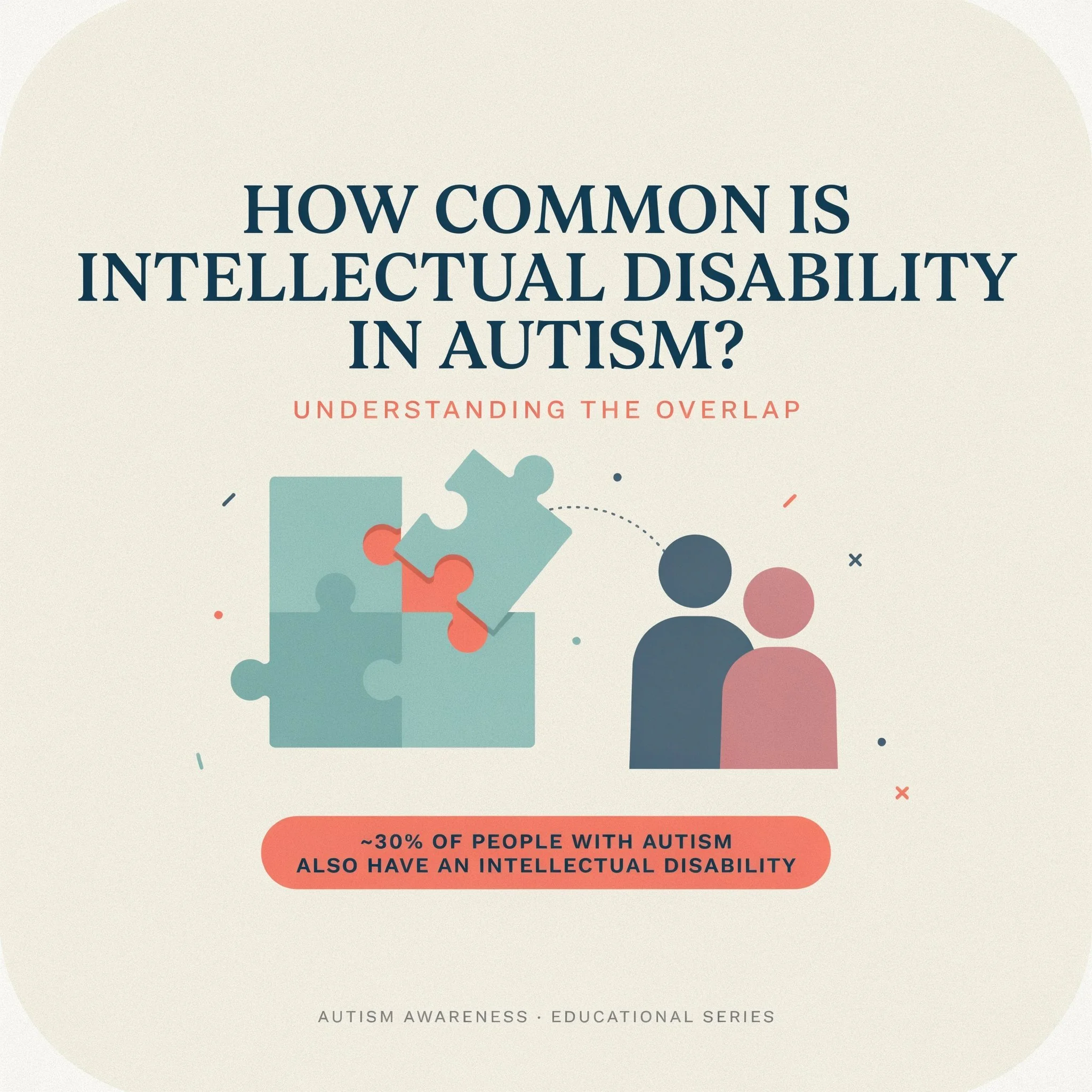
Common intellectual disability in autism
How Common Is Intellectual Disability in Autism?
The research on how common intellectual disability is in autism has produced varying estimates over the years, and understanding those variations helps parents make sense of conflicting information.
Earlier estimates suggested that around 70 to 75 percent of autistic people had intellectual disability. More recent research puts the figure significantly lower, at around 30 to 40 percent. This shift reflects several things.
First, diagnostic criteria for autism have broadened significantly since the 1990s, particularly with the inclusion of Asperger Syndrome in the DSM-4 and the subsequent shift to a single autism spectrum diagnosis in the DSM-5. The broader the diagnostic criteria, the more autistic people without intellectual disability are captured in prevalence data.
Second, better assessment tools have improved the accuracy of cognitive testing in autistic individuals. Earlier IQ assessments were often poorly adapted for autistic people, particularly those who were nonverbal or who had significant communication differences, and may have underestimated intellectual ability.
Third, awareness of autism without intellectual disability has increased significantly, leading to more diagnoses in this population and shifting the overall proportion.
The current best estimate is that approximately 30 to 40 percent of autistic people have a co-occurring intellectual disability. The majority, 60 to 70 percent, do not.
Why Is Autism So Often Confused With Intellectual Disability?
The confusion between autism and intellectual disability has several sources and understanding them helps parents recognize when assumptions are being made about their child that may not be accurate.
Historical reasons: Early autism research focused primarily on autistic individuals with significant support needs, many of whom also had intellectual disability. The image of autism that emerged from that research was heavily shaped by this population, creating an association between autism and intellectual disability that persisted long after research demonstrated the full breadth of the spectrum.
Communication differences: Many autistic children, particularly young autistic children and those who are nonverbal or minimally verbal, present in ways that can look like intellectual disability to observers who are not trained to distinguish the two. A child who does not respond to questions, who does not make eye contact, and who does not engage in typical social interaction may be assumed to have limited intelligence when the actual issue is communication and social differences, not cognitive limitation.
Assessment challenges: Standard intelligence tests are not always well-suited to autistic individuals. They typically require verbal responses, social engagement, and the ability to demonstrate knowledge through neurotypical channels. An autistic child who has significant knowledge and cognitive ability but cannot demonstrate it through standard testing channels may receive a lower IQ score than accurately reflects their ability.
Behavior misinterpretation: Autistic behaviors including limited eye contact, scripted language, repetitive movements, and unusual responses to social situations are sometimes misread as signs of intellectual limitation by people who do not understand autism.
The Problem With Assuming Intellectual Disability in Autism
This section matters as much as any other in this post because the assumption that is autism an intellectual disability translates to yes carries real and harmful consequences for autistic children.
When intellectual disability is assumed in an autistic child who does not have it, several things happen:
Educational placements become inappropriate: Children are placed in settings designed for intellectual disability rather than autism. The curriculum is pitched below their actual cognitive level. Expectations are lowered in ways that become self-fulfilling.
Communication is not pursued: When a child is assumed to have intellectual disability, the investment in finding their communication channel is often reduced. The assumption that they cannot communicate becomes the barrier to discovering that they can.
Strengths are overlooked: The deficit-focused lens of intellectual disability obscures the genuine cognitive strengths that many autistic people have. Pattern recognition, attention to detail, deep focused thinking, and exceptional memory in areas of interest are all common autistic cognitive profiles that are invisible when intellectual disability is assumed.
Self-concept is damaged: Children who are consistently treated as less capable than they are internalize that treatment. The damage to self-esteem and self-concept that comes from years of being underestimated is real, significant, and often persists long after the underestimation is corrected.
How This Connects to Profound Autism
The overlap between autism and intellectual disability is most significant at the most complex end of the autism spectrum. The concept of profound autism, which describes autistic individuals with both significant intellectual disability and minimal or no functional spoken language, is directly relevant to the question of is autism an intellectual disability.
For a full understanding of what profound autism is, how it differs from other autism presentations, and what support looks like for this population, the posts on what is profound autism and profound autism vs autism level 3 cover the topic comprehensively.
FAQs
Can you be autistic and have an intellectual disability?
Yes. Research suggests around 30 to 40 percent of autistic people have a co-occurring intellectual disability.
What percentage of autistic people have intellectual disability?
Current research estimates that approximately 30 to 40 percent of autistic people have a co-occurring intellectual disability meaning the majority do not.
Can an autistic child have a high IQ?
Yes. Many autistic people have average, above average, or exceptionally high IQ scores. High intelligence and autism are not mutually exclusive.
How is intelligence tested in autistic children? Standard intelligence tests are used alongside nonverbal assessments for children with communication differences. Subtest profiles are important because autistic children often show highly variable performance across different cognitive domains.
Does having autism mean my child will need lifelong support? Support needs in autism vary enormously. Some autistic people require minimal support as adults. Others need significant ongoing support. The presence or absence of intellectual disability is one factor among many that affects long-term support needs.
Final Thoughts
Is autism an intellectual disability? No. They are two separate conditions that can and do co-occur but that are distinct in their definitions, their neurological underpinnings, and their implications for support.
Understanding this distinction matters practically. It matters for how autistic children are assessed, how they are placed in educational settings, what expectations are held for them, and what opportunities are made available to them.
The assumption that is autism an intellectual disability answers yes has cost too many autistic people too many years of being underestimated, under-supported, and denied access to the cognitive and communicative channels that could have shown the world what they were actually capable of.
Your child's autism does not define their intelligence. Their autism defines how their brain is organized, how they process information, how they experience the world, and what kind of support they need to thrive in it. Those are very different things from intellectual ability, and treating them as the same thing is a mistake with consequences.
Know the difference. Advocate accordingly. And hold the highest genuinely appropriate expectations for your child at every stage of their journey.
References:
National Institute of Mental Health. Autism Spectrum Disorder [Internet]. Last reviewed December 2024. Available from: https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd
National Academies of Sciences, Engineering, and Medicine. Clinical Characteristics of Intellectual Disabilities. In: Boat TF, Wu JT, editors. Mental Disorders and Disabilities Among Low-Income Children. Washington (DC): National Academies Press (US); 2015. Available from: https://www.ncbi.nlm.nih.gov/books/NBK332877/
de Brito Wanderley D, Muratori F, Argollo N, Tolentino A, Miranda T, Vaz F, Campos V, Marques de Mattos A, Lucena R. Autistic Children and Adolescents Without Intellectual Disability: Individual and Family Profile. Clin Neuropsychiatry. 2025;22(3):215-228. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12302814/
Srivastava AK, Schwartz CE. Intellectual disability and autism spectrum disorders: causal genes and molecular mechanisms. Neurosci Biobehav Rev. 2014;46(2):161-174. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4185273/
Congressional Research Service. The Individuals with Disabilities Education Act (IDEA), Part B: Key Statutory and Regulatory Provisions [Internet]. Report R41833. Available from: https://www.congress.gov/crs-product/R41833
Russell G, Mandy W, Elliott D, White R, Pittwood T, Ford T. Selection bias on intellectual ability in autism research: a cross-sectional review and meta-analysis. Mol Autism. 2019;10:9. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6397505/
Autism Speaks. Autism diagnostic criteria: DSM-5 [Internet]. Available from: https://www.autismspeaks.org/autism-diagnostic-criteria-dsm-5

Early Autism Detection: What Happens When Autism Is Caught Early
Early autism detection is one of the most important factors in determining the quality of life an autistic child will go on to experience. When autism is caught early, the right support can be put in place during the period when the brain is most responsive to intervention, connections can be built before gaps become entrenched, and families can stop guessing and start understanding.
When autism is caught early, everything changes. Not because autism itself changes, the neurology is present from birth and it does not disappear with early identification, but because the environment around the child changes. The support arrives sooner. The misunderstandings are fewer. The years spent confused about why things feel so hard are replaced with years spent learning how to work with the brain your child has rather than against it.
This post covers what the research says about early autism detection, what early intervention actually involves, what parents should watch for, and why the question of when autism is identified matters as much as it does.
Table of Contents
What Early Autism Detection Actually Means
Why Timing Matters: What the Brain Research Says
What Happens When Autism Is Caught Early
Early Signs Parents Should Know
The Earliest Age Autism Can Be Detected
What Early Intervention Looks Like
Barriers to Early Autism Detection
What Parents Can Do Right Now
How Early Detection Connects to Acceptance
FAQs
Final Thoughts
What Early Autism Detection Actually Means
Early autism detection refers to the identification of autism during the earliest possible developmental window, ideally before the age of three and in many cases as early as 18 months. It is the process of recognizing the signs of autism, pursuing evaluation, receiving a diagnosis, and beginning appropriate support before the typical developmental period has passed.
Early autism detection does not mean catching something before it gets worse in the way that early cancer detection does. Autism is not a progressive disease. It does not get worse if it goes undetected. But the opportunities that early autism detection opens up are genuinely time-sensitive in ways that make the timing of identification practically significant.
Early autism detection matters because the brain of a young child is far more plastic and responsive to environmental input than the brain of an older child or an adult. The early years are when the neural connections that support communication, social engagement, sensory regulation, and learning are being most actively formed. When the right support is in place during that window, those connections develop in ways that serve the autistic child far better than they would without support.
Early autism detection is not about changing who an autistic child is. It is about giving their neurology the right conditions to develop as fully and as functionally as possible during the period when development is most responsive to those conditions.
Why Timing Matters: What the Brain Research Says
The neuroscience behind early autism detection is both compelling and straightforward. The brain of a child under three is undergoing a period of extraordinary development. Neural connections are being formed at a rate that will never be matched again in life. The brain is literally constructing itself based on the input it receives from the environment.
This is what neuroscientists call neuroplasticity, and it is at its most powerful in the earliest years of life. The practical implication for autism is significant: when the right support is introduced during this period, the developing brain can build more functional pathways for communication, social engagement, and sensory regulation than it would build without that support.
Research consistently demonstrates that children who receive early autism intervention, particularly before the age of three, show better outcomes across multiple domains including language development, social skills, adaptive functioning, and cognitive development compared to children who receive the same intervention later.
A study found that intensive early intervention significantly improved outcomes for autistic toddlers, with many children making gains that would not have been possible if intervention had begun at school age. Multiple subsequent studies have replicated and extended these findings.
This does not mean that intervention after the early years is ineffective. It absolutely is effective. But the window of maximum neurological responsiveness is real and early autism detection is what opens access to it.

Early autism intervention works
What Happens When Autism Is Caught Early
When autism is caught early the outcomes for autistic children are measurably better across nearly every domain that matters for long-term quality of life.
Language and communication: When autism is caught early and communication support begins during the critical language development window, children develop stronger functional communication skills. This includes both verbal language and alternative communication methods for children who are nonverbal. Early speech and language therapy can make a profound difference to a child's ability to communicate their needs, preferences, and experiences.
Social development: When autism is caught early, support can be tailored to help autistic children develop social skills and build relationships during the period when the social brain is most actively developing. This does not mean making autistic children perform neurotypical social behavior. It means helping them develop authentic ways of connecting with others that work with their neurology.
Sensory regulation: When autism is caught early, occupational therapy and sensory integration support can help children develop more effective sensory regulation strategies during the period when those strategies are most readily learned. Children who develop better sensory regulation early are less likely to experience the kind of sensory overload that significantly affects functioning at school and in the community.
Academic readiness: When autism is caught early, children enter school with more of the foundational skills they need to benefit from education. Communication, self-regulation, attention, and the ability to manage transitions all contribute to school readiness and all can be meaningfully supported through early intervention.
Family functioning: When autism is caught early, families understand what they are dealing with earlier. The confusion, the self-blame, the wondering what is wrong, and the misinterpretation of autistic behavior as intentional or willful all reduce when there is a diagnosis and a framework for understanding the child. Families can access support, connect with community, and build their own knowledge and confidence much sooner.
Mental health: When autism is caught early, the years of struggling without understanding are shorter. Many autistic adults who were diagnosed late report significant mental health impacts from years of not understanding why they were different and why things that seemed easy for others felt so hard. Early autism detection reduces the duration of that confusion.
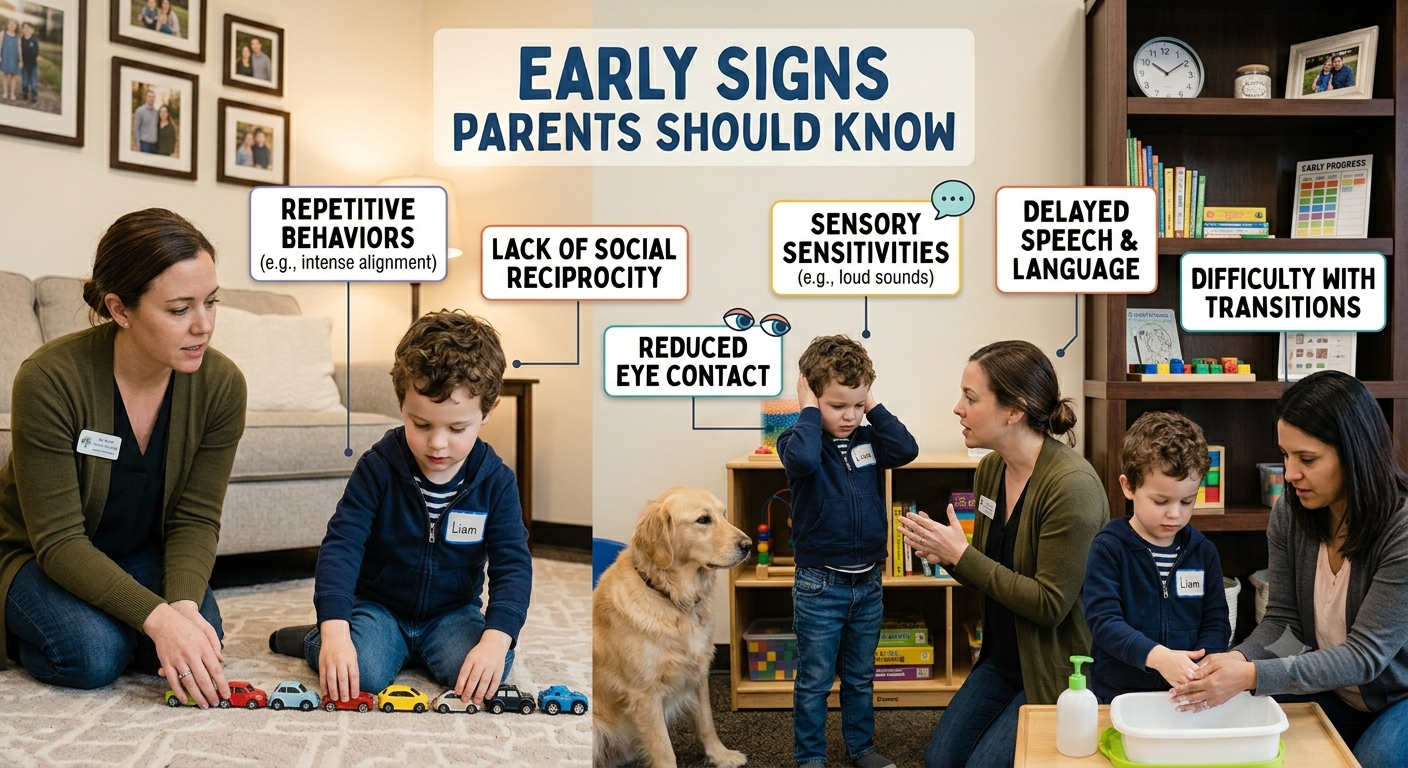
Autism Signs
Early Signs Parents Should Know
Knowing the early signs of autism is part of early autism detection and it is something every parent benefits from understanding whether or not they currently have concerns about their child.
Signs in the first year:
Limited eye contact during feeding and social interaction
Not responding to their name by 9 to 12 months
Not showing things to parents by pointing by 12 months
Limited babbling or loss of babbling that had been developing
Not reaching toward familiar people
Unusual responses to sensory input including sounds, touch, or lights
Signs between 12 and 24 months:
Not using single words by 16 months
Not using two-word phrases by 24 months
Loss of previously acquired language at any point
Not engaging in simple pretend play by 18 months
Limited interest in other children
Strong preference for specific routines with significant distress at changes
Repetitive movements including hand flapping, spinning, or rocking
Intense focus on specific objects or aspects of objects
Signs in the preschool years:
Significant difficulty with peer interaction
Unusual language patterns including echolalia, scripted speech, or very formal language
Extreme reactions to sensory input
Intense, narrow interests that dominate play
Difficulty with transitions and unexpected changes
Limited pretend play or play that is highly repetitive
The presence of any of these signs does not confirm autism. But it does mean that seeking evaluation is the right next step. For a complete guide to the testing process once concerns have been identified, the post on how to test for autism covers every stage in detail.

Ages autism can be detected
The Earliest Age Autism Can Be Detected
Early autism detection has its limits, and those limits are worth understanding honestly.
The American Academy of Pediatrics recommends autism-specific screening at 18 and 24 months. Research suggests that reliable autism identification is possible from around 18 months for children showing clear signs and from 24 months for more subtle presentations.
Some research has found that certain early markers in infant behavior, including patterns of eye contact, response to name, and social engagement, can be detectable as early as six months in infants who are later diagnosed with autism. These very early markers are currently the subject of active research but are not yet used in routine clinical screening.
For most families, the realistic window for early autism detection begins between 18 and 24 months when standard screening tools are reliable and diagnostic evaluations can be conducted with confidence.
It is worth noting that even an 18 to 24 month diagnosis, while considered early in clinical terms, still allows access to early intervention services during the most critical developmental window. Early is relative, and any diagnosis before school age opens doors that later diagnosis does not.
For parents who are carrying the emotional weight of a new diagnosis and trying to find their footing between the urgency of early intervention and the importance of acceptance, Sonia's coaching work is built for exactly that balance.
Book a coaching session with Sonia here and get the support that helps you hold both the urgency and the acceptance at the same time.
What Early Intervention Looks Like
Early autism detection is only valuable if it is followed by early intervention. Understanding what early intervention actually involves helps parents know what to pursue and what to expect.
Speech and language therapy: Communication support is almost universally recommended as part of early intervention for autistic children. This includes verbal language development for children who are developing speech and AAC implementation for children who are nonverbal or minimally verbal. Early speech therapy during the critical language development window is one of the most impactful interventions available.
Occupational therapy: Occupational therapy in early intervention addresses sensory processing, fine motor development, and the daily living skills that autistic children may need specific support to develop. Sensory integration approaches help young autistic children develop more effective regulation strategies during the period when those strategies are most readily learned.
Applied Behavior Analysis: ABA therapy is widely used in early autism intervention and has the most extensive evidence base of any autism intervention approach. It is also the most debated, with significant concerns raised by autistic advocates about historical ABA practices focused on compliance and suppression of autistic traits. Modern naturalistic ABA approaches that focus on skill development in the context of play and child-led interaction are generally considered more appropriate than older discrete trial formats.
Developmental relationship-based approaches: Approaches including DIR Floortime and the Early Start Denver Model use child-led play and relationship-based interaction to support communication, social engagement, and development. These approaches have growing evidence bases and are widely endorsed by autistic advocates as more affirming than purely behavioral approaches.
Early childhood special education: Many children with early autism detection qualify for early childhood special education services through their school district beginning at age three. These services provide structured educational support in settings designed for children with developmental needs.
Parent coaching: One of the most impactful components of early intervention is supporting parents to understand their child's communication and developmental needs and to respond in ways that promote development in everyday interactions. Parent coaching multiplies the impact of formal therapy by extending support into every interaction throughout the child's day.
Barriers to Early Autism Detection
Early autism detection is not equally available to all families and the barriers that prevent it are worth naming clearly.
Racial and ethnic disparities:Research consistently shows that Black, Hispanic, and Asian children are diagnosed with autism later on average than white children. These disparities reflect systemic inequities in access to healthcare, cultural factors that affect how autistic behavior is interpreted, and bias in the referral and diagnostic process.
Geographic barriers: Families in rural and remote areas often face significant barriers to autism evaluation including limited availability of specialist services and long travel distances to evaluation centers.
Economic barriers: Comprehensive private autism evaluations can cost several thousand dollars. Public pathways exist but have long waiting lists in many areas. Families without resources to access private evaluation may wait significantly longer for diagnosis.
Cultural barriers: In some communities, autism is stigmatized in ways that prevent families from seeking evaluation. Cultural beliefs about the cause of developmental differences, distrust of medical systems, and concerns about labeling can all delay early autism detection.
Professional barriers: Not all pediatricians are equally knowledgeable about autism. Concerns raised by parents are sometimes dismissed, minimized, or attributed to parenting anxiety. Families of girls are particularly likely to encounter this barrier.
Addressing these barriers is a systemic issue that goes beyond what individual families can solve. But knowing they exist helps parents advocate more effectively when they encounter them.
What Parents Can Do Right Now
If you are concerned about your child's development, here is what to do:
Request autism screening at your child's next pediatric appointment, or sooner if concerns are present
Document specific behaviors you have observed with dates and contexts
Request a referral for a full autism evaluation if screening raises concerns or if you have concerns regardless of screening results
Contact your local early intervention program directly if your child is under three, you do not need a referral in most states
Request a free educational evaluation through your school district if your child is three or older
Connect with other autism families who can share their experience navigating the evaluation and early intervention process
How Early Detection Connects to Acceptance
Early autism detection is most valuable when it is followed not just by early intervention but by early acceptance.
The goal of early identification is not to minimize autism or to engineer the most neurotypical version of the autistic child possible. It is to understand the child deeply enough, early enough, to build a life and an environment that genuinely supports them.
That requires acceptance alongside intervention. Acceptance of the autistic neurology as the genuine, permanent, valuable foundation of who your child is. Acceptance that the goal is flourishing as an autistic person, not passing as a neurotypical one.
The post on autism awareness vs autism acceptance covers why that distinction matters and what acceptance looks like in practice. It is worth reading early in the journey because the framework you bring to your child's diagnosis shapes every decision you make from here.
FAQs
What does it mean when autism is caught early
Early autism detection means identifying autism before age three when the brain is most responsive to intervention and support can be put in place during the critical developmental window.
What happens when autism is caught early?
When autism is caught early children show better outcomes in communication, social development, sensory regulation, school readiness, and mental health compared to children identified later.
Can autism be detected at birth?
Not reliably. Early markers may be present in the first months of life but reliable identification typically begins around 18 months using validated screening tools.
Does early detection mean early intervention always works? Early intervention significantly improves outcomes but results vary depending on the individual child, the type of intervention, and the quality of support provided.
What is the best early intervention for autism?
No single approach works for every child. Speech therapy, occupational therapy, developmental relationship-based approaches, and parent coaching all have strong evidence bases for early intervention.
Does early autism detection change the autism itself?
No. Autism is neurological and present from birth. Early detection changes the support environment, not the underlying neurology.
Does early autism detection prevent autism regression?
Early detection and appropriate support reduce the risk of autism regression by building stronger regulatory and communicative foundations before the demands that trigger regression become significant.
Final Thoughts
Early autism detection is not about fear. It is not about catching something terrible before it gets worse. It is about giving an autistic child the right conditions at the right time, during the window when those conditions make the most difference to how their brain develops and how their life unfolds.
When autism is caught early, families stop guessing and start understanding. Children stop struggling in silence and start receiving support that makes sense of their experience. The years of confusion are shorter. The foundation is stronger. The path forward is clearer.
If you have concerns about your child's development, act on them now. The evaluation process is navigable. The early intervention services are accessible. And the difference that early autism detection makes to a child's life is real, measurable, and worth every step of the process it takes to get there.
Your child's brain is working hard. Early autism detection is how you make sure the world works with it.
References:
Maksimović S, Marisavljević M, Stanojević N, Ćirović M, Punišić S, Adamović T, Đorđević J, Krgović I, Subotić M. Importance of Early Intervention in Reducing Autistic Symptoms and Speech–Language Deficits in Children with Autism Spectrum Disorder. Children (Basel). 2023 Jan 6;10(1):122. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9857540/
Estes A, Munson J, Rogers SJ, Greenson J, Winter J, Dawson G. Long-Term Outcomes of Early Intervention in 6-Year-Old Children With Autism Spectrum Disorder. J Am Acad Child Adolesc Psychiatry. 2015 Jul;54(7):580-7. Available from: https://pubmed.ncbi.nlm.nih.gov/26088663/
American Academy of Pediatrics. Autism Spectrum Disorder [Internet]. Last updated October 2025. Available from: https://www.aap.org/en/patient-care/autism/
Young GS, Merin N, Rogers SJ, Ozonoff S. Gaze Behavior and Affect at 6-Months: Predicting Clinical Outcomes and Language Development in Typically Developing Infants and Infants At-Risk for Autism. Dev Sci. 2009 Sep;12(5):798-814. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2732664/
International Council on Development and Learning (ICDL). What is DIR®? [Internet]. Available from: https://www.icdl.com/dir
Autism Speaks. What is Early Start Denver Model (ESDM)? [Internet]. Available from: https://www.autismspeaks.org/early-start-denver-model-esdm
Aylward BS, Gal-Szabo DE, Taraman S. Racial, Ethnic, and Sociodemographic Disparities in Diagnosis of Children with Autism Spectrum Disorder. J Dev Behav Pediatr. 2021 Oct-Nov;42(8):682-689. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8500365/

How to Test for Autism: A Complete Guide for Parents
If you are wondering how to test for autism, you are probably not reading this out of idle curiosity. You are reading it because something has shifted. A developmental checkup raised a concern. A teacher said something. A friend mentioned it. Or you have been watching your child and quietly noting things that do not quite add up, and you have finally decided to find out what is going on.
Knowing how to test for autism is the first practical step in a process that can feel overwhelming before you understand how it actually works. This post walks you through everything, from the earliest screening tools to the full diagnostic process, what to expect at each stage, how to advocate effectively, and what comes after a diagnosis.
How to test for autism is a question with a real, practical answer. And having that answer puts you in a far stronger position than most parents have when they start this process.
So, let’s get into it.
Table of Contents
How to Test for Autism: The Short Answer
The Difference Between Autism Screening and Autism Testing
Early Signs That Prompt Autism Testing
Step One: Developmental Screening at Your Pediatrician
Step Two: Formal Autism Evaluation
Who Can Diagnose Autism
What Happens During an Autism Evaluation
The Main Diagnostic Tools Used to Test for Autism
Online Autism Tests: Are They Reliable
What Happens After an Autism Diagnosis
How to Advocate for Testing When You Are Being Dismissed
Final Thoughts
How to Test for Autism: The Short Answer
How to test for autism involves a two-stage process. The first stage is screening, which identifies children who may be at risk for autism and need further evaluation. The second stage is a comprehensive diagnostic evaluation, which is a detailed, multi-professional assessment that either confirms or rules out an autism diagnosis.
There is no single test for autism. No blood test, no brain scan, no genetic test, and no quick checklist can diagnose autism on its own. Autism is diagnosed through a combination of developmental history, behavioral observation, standardized assessment tools, and clinical judgment from trained professionals.
This two-stage process is how to test for autism in the most accurate and reliable way currently available. Understanding both stages and what happens within them helps parents navigate the process with confidence rather than confusion.
The Difference Between Autism Screening and Autism Testing
Before going further, it helps to understand that screening and testing are different things and the distinction matters practically.
Autism screening: Screening is a quick, low-burden process designed to identify children who may need further evaluation. It does not diagnose autism. It flags a concern and prompts the next step. Screening tools are typically used by pediatricians at routine developmental checkups and take only a few minutes to complete.
Autism testing or evaluation: A full autism evaluation is a comprehensive, multi-session process conducted by trained specialists. It involves direct observation of the child, standardized assessment tools, detailed developmental history, and input from multiple sources including parents, teachers, and other professionals who know the child. It results in either a diagnosis or a ruling out of autism, along with a full picture of the child's strengths and support needs.
The screening identifies who needs testing. The testing provides the diagnosis.

early signs of autism to know
Early Signs That Prompt Autism Testing
Most parents begin thinking about how to test for autism because they have noticed something specific about their child's development. Here are the signs that most commonly prompt parents and professionals to pursue autism testing:
In infants and toddlers:
Not responding to their name by 12 months
Not pointing or waving by 12 months
No babbling by 12 months
No two-word phrases by 24 months
Loss of previously acquired language or social skills at any age
Limited or absent eye contact
Not smiling in response to smiling faces
Appearing not to hear even though hearing tests are normal
In preschool age children:
Significant difficulty with social interaction with peers
Strong preference for routine with extreme distress at changes
Repetitive movements including hand flapping, rocking, or spinning
Intense, narrow interests that dominate play and conversation
Unusual sensory responses including strong reactions to sounds, textures, or lights
Delayed or unusual language development
Difficulty with pretend play
In school age children:
Social difficulties that are becoming more visible as peer expectations increase
Difficulty understanding unwritten social rules
Challenges with executive functioning including organization and task initiation
Sensory sensitivities that affect participation in school activities
Intense special interests that differ significantly from peers
Difficulty with transitions and unexpected changes
In teenagers:
Social isolation increasing as peer relationships become more complex
Anxiety and depression emerging alongside social difficulty
Academic performance inconsistent with cognitive ability
Fatigue and burnout from sustained social effort
Questioning their own identity and neurological difference
If you are seeing several of these signs in your child, pursuing autism testing is the right next step. Waiting to see if they grow out of it is rarely the best approach. Earlier identification means earlier support, and earlier support produces better outcomes.
Step One: Developmental Screening at Your Pediatrician
The first step in how to test for autism for most families is a conversation with their child's pediatrician.
The American Academy of Pediatrics recommends autism-specific screening for all children at their 18 and 24 month well-child visits, regardless of whether any concerns have been raised. Many pediatricians also screen at other routine visits if developmental concerns are present.
The most widely used screening tool at this stage is the M-CHAT-R, which stands for Modified Checklist for Autism in Toddlers, Revised. It is a 20-item parent-report questionnaire that takes about five minutes to complete and identifies toddlers who may need further evaluation.
What to do at this stage:
Be honest and specific when completing screening questionnaires. Describe what your child actually does, not what you hope or expect they will do
Come prepared with specific examples of the behaviors that concern you
Ask directly whether your child's screening results suggest further evaluation is needed
Request a referral for a full evaluation if the screening is positive or if you have concerns even when the screening is negative
It is worth knowing that a negative screening result does not rule out autism, particularly in children who have developed effective compensatory strategies or whose autism presents in ways that are less visible on standard screening tools. If you have concerns, advocate for further evaluation regardless of screening results.
Step Two: Formal Autism Evaluation
If screening raises concerns or if you have requested a full evaluation based on your own observations, the next step in how to test for autism is a comprehensive diagnostic evaluation.
This evaluation can be requested through several pathways:
Through your pediatrician: Ask for a referral to a developmental pediatrician, child psychologist, or autism specialist for a full evaluation.
Through your school district: Under the Individuals with Disabilities Education Act, you have the right to request a free educational evaluation through your child's school district. This evaluation is not the same as a clinical diagnosis but can identify educational support needs and sometimes contributes to the diagnostic process.
Through a specialist center: Many children's hospitals and university medical centers have dedicated autism evaluation programs. These programs typically offer the most comprehensive evaluations but often have longer waiting lists.
Privately: Private autism evaluations are available through clinical psychologists and developmental pediatricians in private practice. These can be faster than public pathways but involve out of pocket costs that vary significantly.

Professionals who can diagnose autism
Who Can Diagnose Autism
Knowing who can diagnose autism is part of understanding how to test for autism effectively.
In the United States, autism can be diagnosed by:
Developmental pediatricians: Medical doctors who specialize in child development and developmental disorders
Child psychiatrists: Medical doctors who specialize in mental health conditions in children including neurodevelopmental conditions
Clinical psychologists: Doctoral level psychologists with training in psychological assessment and neurodevelopmental conditions
Pediatric neurologists: Medical doctors specializing in neurological conditions in children, particularly relevant when epilepsy or other neurological conditions are also present
The most comprehensive autism evaluations are typically conducted by multidisciplinary teams that include several of these professionals working together. A team approach produces a more complete picture of the child's profile than a single professional assessment.
What Happens During an Autism Evaluation
Understanding what happens during an autism evaluation helps parents prepare effectively and know what to expect. Here is a typical sequence:
Developmental history interview: A detailed interview with parents covering the child's developmental history from birth, including milestones, early language development, social development, behavioral patterns, medical history, and family history. This usually takes one to two hours and is one of the most important parts of the evaluation.
Direct assessment of the child: The evaluator spends direct time with the child conducting standardized observations and assessments. The child may participate in structured play activities, respond to social prompts, complete cognitive tasks, and engage in conversation depending on their age and language level.
Cognitive and language assessment: Most comprehensive autism evaluations include assessment of cognitive ability and language development. This helps identify co-occurring conditions including intellectual disability and language disorders and provides a complete picture of the child's profile.
Behavior rating scales: Standardized questionnaires completed by parents and teachers that assess behavior across different settings. These provide information about how the child functions across environments rather than only in the assessment room.
Sensory processing assessment: Many evaluations include assessment of sensory processing, either through standardized tools or through clinical observation.
Feedback session: After the evaluation is complete, the evaluating team meets with parents to share findings, explain the diagnosis or ruling out of autism, and discuss recommendations for support.
If this section resonated with you, this is exactly what coaching sessions with Sonia are built around. Book here.
The Main Diagnostic Tools Used to Test for Autism
Several standardized tools are commonly used as part of how to test for autism in clinical practice. Knowing what these are helps parents understand the process:
ADOS-2 (Autism Diagnostic Observation Schedule, Second Edition): This is considered the gold standard observational assessment for autism. It is a structured, semi-structured interaction between the evaluator and the child that is scored according to specific criteria. It provides direct observational data on social communication and restricted or repetitive behaviors.
ADI-R (Autism Diagnostic Interview, Revised):A structured interview with parents covering developmental history and current behavior. It is often used alongside the ADOS-2 to provide a comprehensive picture combining observational and historical data.
M-CHAT-R:The screening tool used at pediatric well-child visits for toddlers aged 16 to 30 months.
CARS-2 (Childhood Autism Rating Scale, Second Edition): A rating scale used to assess autism severity across multiple behavioral domains.
Vineland Adaptive Behavior Scales:Assesses adaptive functioning including communication, daily living skills, and socialization across age groups.
Online Autism Tests: Are They Reliable
Parents searching for how to test for autism will inevitably come across online autism tests and screening tools. It is worth being clear about what these are and what they are not.
What online autism tests can do:
Provide an informal indication of whether an autism evaluation might be worthwhile
Help parents organize their observations and concerns before a professional consultation
Give autistic adults a framework for understanding their own experience before seeking formal diagnosis
What online autism tests cannot do:
Diagnose autism
Replace a comprehensive clinical evaluation
Provide a reliable ruling out of autism
The most widely used and most validated online screening tools include the Autism Spectrum Quotient, known as the AQ, developed by Simon Baron-Cohen and colleagues at Cambridge University, and the Ritvo Autism Asperger Diagnostic Scale, known as the RAADS-R. These are research-grade tools that can provide useful information but are not diagnostic instruments.
If an online screening raises concerns, the appropriate next step is a full clinical evaluation with a qualified professional. Online tools are a starting point, not an endpoint.
What Happens After an Autism Diagnosis
Understanding what comes after autism testing and diagnosis is part of knowing how to test for autism effectively because the diagnosis is only the beginning of the process.
After a diagnosis, the immediate priorities are:
Getting the right support in place: Use the diagnosis to access services including speech therapy, occupational therapy, behavioral support, and school accommodations. The diagnosis is the key that unlocks these services.
Educating yourself: Read widely from credible sources including autistic authors and advocates. The more you understand your child's specific profile, the better you can advocate for them and support them.
Connecting with community: Find other families who are navigating similar experiences. The autism parenting community is one of the most generous and knowledgeable communities you will ever encounter.
Processing the emotional response: A diagnosis brings up complex emotions for most parents. Giving yourself space to process those emotions, with support if needed, is important before diving entirely into action mode.
For a comprehensive guide to the practical steps that follow a diagnosis, the post on newly diagnosed autism parent guide covers everything in detail.
For the broader context of what acceptance looks like beyond diagnosis, the post on autism awareness vs autism acceptance is worth reading early in the journey because the framework you use to understand your child's diagnosis will shape every decision you make from here.
How to Advocate for Testing When You Are Being Dismissed
One of the most frustrating experiences parents describe in the autism testing process is being dismissed by professionals who minimize their concerns. Here is how to advocate effectively when that happens:
Document everything: Keep a written record of specific behaviors you have observed, with dates, contexts, and details. Specific documented observations are harder to dismiss than general concerns.
Request things in writing: If a professional declines to refer for evaluation, ask them to put that decision in writing with their clinical reasoning. This often prompts a more careful reconsideration.
Seek a second opinion: You are not obligated to accept a single professional's judgment. If your concerns are being dismissed, seek another opinion from a professional with specific autism expertise.
Use your school district rights: Under IDEA you have the right to request a free educational evaluation through your school district. You do not need your pediatrician's agreement to do this. Submit the request in writing and the school district has 60 days to respond.
Trust your observations: You know your child better than any professional who has spent one hour with them. Your observations are valid data. Do not let a dismissive response convince you otherwise.
Final Thoughts
Knowing how to test for autism puts you ahead of where most parents are when they start this process. The testing itself is not something to fear. It is the process of finally getting accurate information about your child that you can use to get them the support they deserve.
How to test for autism is a question with a clear practical answer. Two stages. Multiple professionals. Standardized tools combined with developmental history and direct observation. A process that takes time but produces a picture of your child that opens doors to genuine support.
If you have concerns about your child, pursue them. Document what you are seeing. Request the evaluation. Advocate when you need to. And trust that the clarity that comes from knowing is almost always better than the uncertainty of not knowing.
Your child is worth finding out.
References:
American Academy of Pediatrics. Autism Spectrum Disorder [Internet]. Last updated October 2025. Available from: https://www.aap.org/en/patient-care/autism/
Robins DL, Fein D, Barton M. M-CHAT-R/F: Modified Checklist for Autism in Toddlers, Revised with Follow-Up [Internet]. 2009. Available from: https://www.mchatscreen.com/
U.S. Department of Education. Individuals with Disabilities Education Act, Section 1414: Evaluations, Eligibility Determinations, Individualized Education Programs, and Educational Placements [Internet]. Available from: https://sites.ed.gov/idea/statute-chapter-33/subchapter-ii/1414/
Global Autism Interactive Network (GAIN), University of Kansas Life Span Institute. Autism Diagnostic Interview – Revised (ADI-R) [Internet]. Available from: https://gain.ku.edu/autism-diagnostic-interview-revised-adi-r
Massachusetts General Hospital, Lurie Center for Autism. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) [Internet]. Available from: https://www.massgeneral.org/children/autism/lurie-center/autism-diagnostic-observation-schedulesecond-edition-ados2
Ji SI, Park H, Yoon SA, Hong SB. A Validation Study of the CARS-2 Compared With the ADOS-2 in the Diagnosis of Autism Spectrum Disorder: A Suggestion for Cutoff Scores. J Korean Acad Child Adolesc Psychiatry. 2023 Jan;34(1):45-50. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9816003/
ScienceDirect Topics. Vineland Adaptive Behavior Scale [Internet]. Elsevier. Available from: https://www.sciencedirect.com/topics/medicine-and-dentistry/vineland-adaptive-behavior-scale
Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The Autism-Spectrum Quotient (AQ): Evidence from Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and Mathematicians. J Autism Dev Disord. 2001;31(1):5-17. Available from: https://psychology-tools.com/test/autism-spectrum-quotient
Ritvo RA, et al. Ritvo Autism Asperger Diagnostic Scale – Revised (RAADS-R) [Internet]. NovoPsych. 2011. Available from: https://novopsych.com/assessments/diagnosis/ritvo-autism-asperger-diagnostic-scale-revised-raads-r/
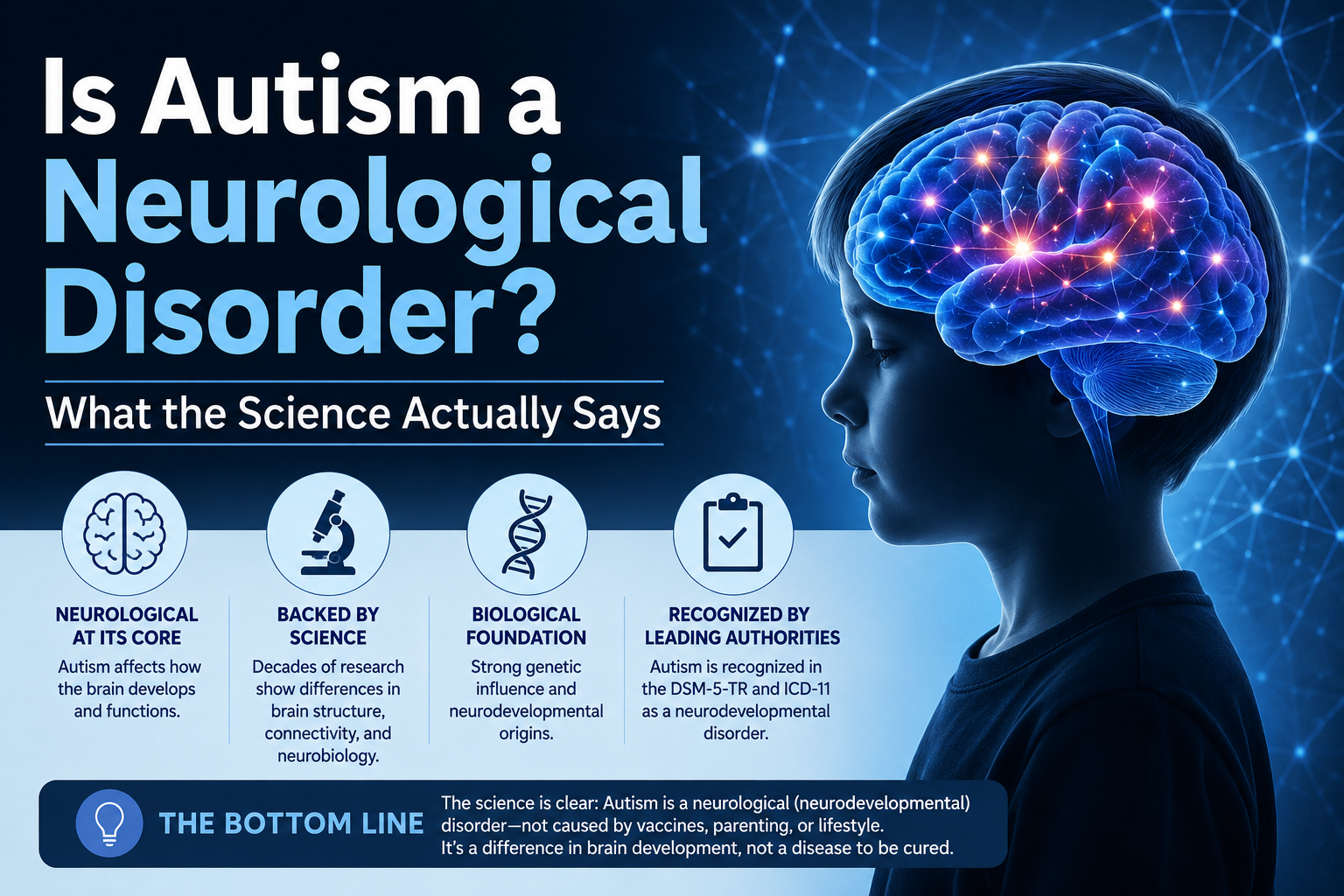
Is Autism a Neurological Disorder? What the Science Actually Says
Is autism a neurological disorder is one of the most searched questions about autism in the United States right now. And it is a question that deserves a careful, honest answer because the way it gets answered shapes how autistic people are seen, how they are treated, and how they see themselves.
Is autism a neurological disorder is not a simple yes or no question. It sits at the intersection of neuroscience, medical classification, identity politics, and lived experience. Getting it right matters not just academically but practically, for the families navigating a diagnosis, for the autistic adults trying to understand their own neurology, and for the professionals and systems that are supposed to support them.
This post answers the question is autism a neurological disorder directly and honestly, explains what the science actually says, covers why the framing of the question matters, and gives parents and autistic adults the context they need to think clearly about what a diagnosis actually means.
Table of Contents
Is Autism a Neurological Disorder: The Direct Answer
What Neurological Actually Means
What the Brain Research Says About Autism
What Causes Autism Neurologically
How Autism Affects the Brain Differently at Different Levels
Why the Disorder vs Difference Debate Matters for Support
How This Connects to High Functioning Autism and Autism Regression
FAQs
Final Thoughts
Is Autism a Neurological Disorder?
Is autism a neurological disorder? Yes, in the sense that autism originates in the brain and nervous system and involves differences in how the brain is structured and how it functions. The neurology of autistic people is genuinely different from the neurology of neurotypical people in ways that are measurable, observable, and consistent across the autistic population.
But is autism a neurological disorder in the sense that something has gone wrong, that the brain is broken, that the difference is inherently a deficit? That is where the answer becomes more complicated and more contested.
Is autism a neurological disorder is a question that science answers one way and the autism community answers in several different ways simultaneously. Understanding both of those answers and why they differ is essential for anyone trying to make sense of what an autism diagnosis actually means.
The short version: autism is neurological. Whether it is accurately described as a disorder depends on which framework you are using to define disorder and whose experience you are centering when you make that judgment.

What Neurological Actually Means
Before going further into whether is autism a neurological disorder, it helps to be clear about what neurological actually means.
Neurological refers to anything that originates in or involves the nervous system, which includes the brain, the spinal cord, and the network of nerves throughout the body. A neurological condition is one whose primary cause and primary effects are located in the nervous system.
Neurological conditions include epilepsy, Parkinson's disease, multiple sclerosis, and migraines. They also include conditions like dyslexia, ADHD, and autism. What these conditions share is that their primary characteristics arise from differences in how the nervous system is structured or how it functions, rather than from external injury, infection, or purely psychological causes.
By this definition, autism is clearly neurological. The characteristics of autism, differences in social communication, sensory processing, information processing, and behavioral regulation, all arise from differences in brain structure and function. They are not caused by external events, bad parenting, or psychological conflicts. They are built into the neurology of the autistic person.
Whether that neurological difference constitutes a disorder is the question that generates most of the debate.
What the Brain Research Says About Autism
The neuroscience of autism has advanced significantly over the past two decades and the findings are genuinely fascinating. Here is what the research tells us about how autistic brains differ from neurotypical brains:
Structural differences:
Research using brain imaging has identified several consistent structural differences in autistic brains compared to neurotypical brains. These include differences in the size and connectivity of the amygdala, which is involved in emotional processing and threat detection, differences in the prefrontal cortex, which is involved in executive functioning and social cognition, and differences in the corpus callosum, which connects the two hemispheres of the brain.
Connectivity differences:
One of the most consistent findings in autism neuroscience is that autistic brains show different patterns of connectivity than neurotypical brains. Some areas show increased local connectivity, meaning stronger connections within specific brain regions, while long range connectivity between distant brain regions is often reduced. This connectivity pattern may help explain both the intense focus and pattern recognition that characterizes many autistic individuals and the difficulties with integrating information across different brain systems.
Sensory processing differences:
Autistic brains process sensory information differently from neurotypical brains. Research has found differences in how the autistic brain filters, prioritizes, and integrates sensory input. The autistic nervous system often does not apply the same predictive filtering that neurotypical nervous systems use to manage the constant flood of sensory information from the environment. The result is a sensory experience that is often more intense, less filtered, and more demanding of cognitive resources.
Mirror neuron differences:
Also, research has suggested differences in mirror neuron system functioning in autism, which may relate to the social communication differences that characterize the condition. This research is ongoing and debated but points toward neurological underpinnings of the social differences in autism.
Neuroinflammation:
Research has found evidence of neuroinflammation in autistic brains, particularly in individuals with more significant support needs. This is an active area of research and its implications for understanding autism are still being worked out.
What all of this research confirms is that autism is neurological. The differences are real, measurable, and present from birth. They are not acquired, not caused by environmental factors after birth, and not the result of developmental failure in the simple sense.
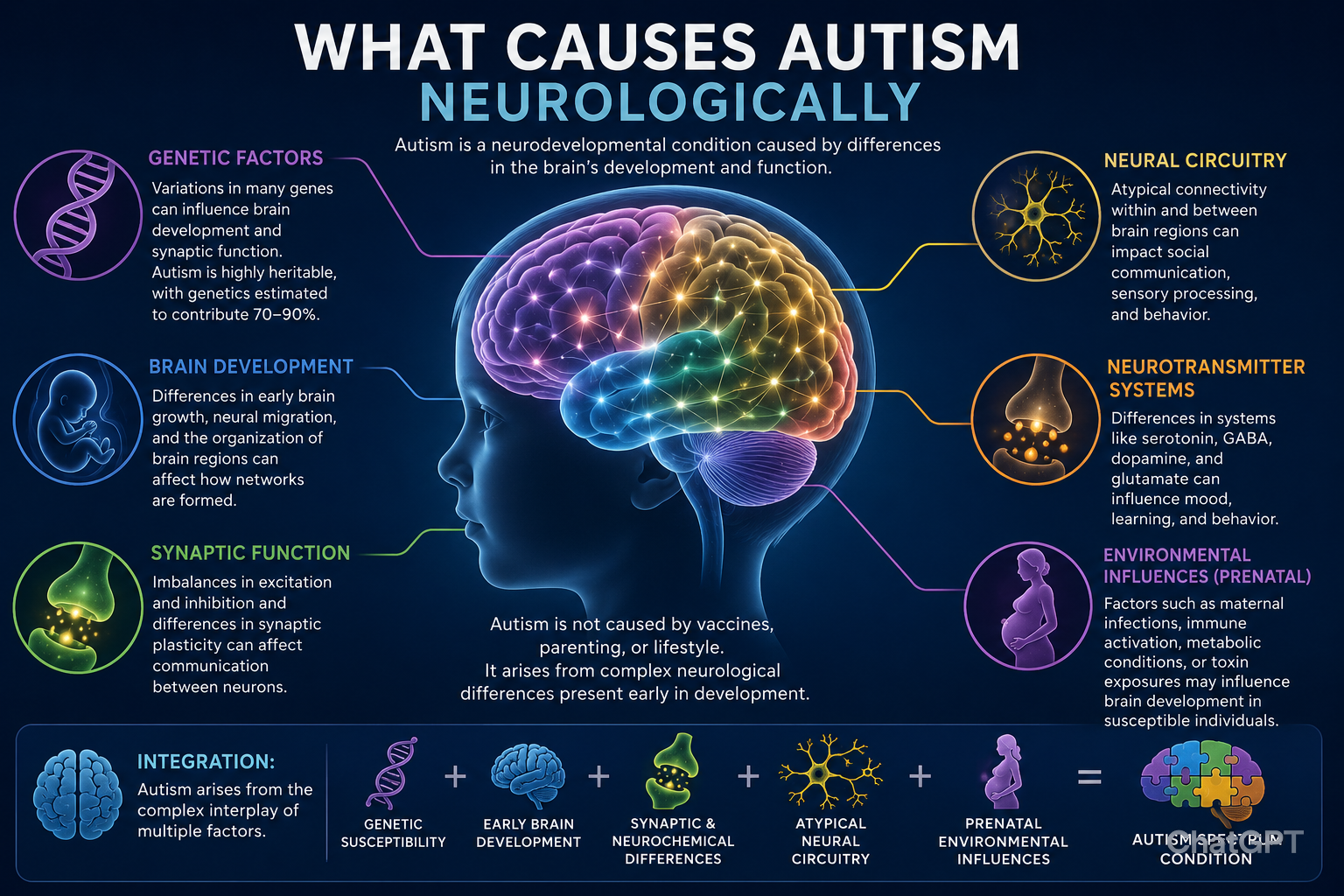
What Causes Autism Neurologically
At a neurological level, autism is caused by differences in brain development that begin during fetal development and continue through early childhood. These developmental differences affect the structure, connectivity, and functioning of the brain in the ways described in the brain research section above.
The specific neurological mechanisms underlying autism are still being actively researched. Current understanding points toward:
Differences in synaptic development and pruning, the process by which neural connections are formed and refined during development
Differences in the balance between excitatory and inhibitory neural signaling
Differences in the development of neural circuits involved in social cognition, sensory processing, and executive functioning
Possible differences in neuroinflammatory processes during early brain development
None of these mechanisms represent simple damage or deficiency. They represent a different developmental trajectory that produces a differently organized brain. Understanding this helps move away from the deficit model of autism toward a model that can acknowledge both the genuine challenges autism creates and the genuine strengths it produces.
The self-esteem coaching Sonia offers is particularly relevant for autistic adults who wants to build a stable, grounded sense of identity that starts from an accurate understanding of your own neurology is genuinely transformative wor.
Book a self-esteem coaching session with Sonia here.
How Autism Affects the Brain Differently at Different Levels
One of the most important things to understand about autism neuroscience is that the brain differences associated with autism are not uniform across the spectrum. The neurology of a profoundly autistic individual with significant intellectual disability and no functional spoken language looks meaningfully different from the neurology of an autistic individual with average intelligence and functional language.
This neurological variability is one of the reasons the autism spectrum is a spectrum rather than a single unified condition. The shared features across the spectrum, differences in social communication and restricted or repetitive behaviors, arise from related but not identical neurological profiles.
At the more complex end of the spectrum, the neurological differences tend to be more pervasive, affecting more brain systems and producing more significant impairments in daily functioning. Co-occurring neurological conditions including epilepsy are more common. The connectivity differences tend to be more pronounced.
At the less complex end of the spectrum, the neurological differences may be more subtle and more localized, affecting specific brain systems in ways that produce significant challenges in some areas while leaving others relatively intact.
Understanding this variability is essential for making sense of why autism looks so different across individuals and why what works as support for one autistic person may not work for another.
For a full breakdown of how autism presents across different levels and what those differences mean for support, the post on what is high functioning autism covers the less visible end of the spectrum in depth.
Why the Disorder vs Difference Debate Matters for Support
The debate about whether is autism a neurological disorder or a neurological difference is not just academic. It has direct practical implications for how autistic people are supported.
If autism is primarily framed as a disorder: Support focuses on reducing autistic traits, building skills that allow autistic people to function more like neurotypical people, and treating the deficits that autism creates. The goal is normalization.
If autism is primarily framed as a difference: Support focuses on accommodating autistic neurology, building on autistic strengths, removing environmental barriers, and helping autistic people thrive as their authentic selves. The goal is flourishing.
The evidence strongly supports the second approach producing better long-term outcomes for most autistic people. Approaches that focus on making autistic people appear more neurotypical without addressing their actual needs tend to produce increased masking, increased anxiety, and increased risk of autistic burnout.
This is exactly the framework that informs the coaching work Sonia does with neurodivergent individuals. The goal is never to make an autistic person more neurotypical. It is to help them understand their own neurology deeply enough to build a life that genuinely works for them.
Book a socio-emotional coaching session with Sonia here and experience what support built around your actual neurology feels like.
How This Connects to High Functioning Autism and Autism Regression
The neurological framework for understanding autism connects directly to two of the most important practical topics for parents and autistic adults.
High functioning autism is often described as if functioning is a fixed characteristic of the autistic person. The neuroscience tells a different story. Functioning in autism is highly context dependent and is significantly affected by environmental demands, sensory load, anxiety levels, and the degree to which the autistic person is masking. A person who is described as high functioning is not neurologically different from a person who is struggling. They are often the same neurology under different conditions.
For a full understanding of what high functioning autism actually means and what the neuroscience behind it tells us about support needs, the post on what is high functioning autism is essential reading.
Autism regression is neurologically explainable within the framework this post has outlined. When an autistic nervous system is pushed beyond its regulatory capacity, whether through masking, environmental demands, sensory overload, or medical factors, the result can be a loss of previously acquired skills. This is not a sign of neurological deterioration. It is a sign of a nervous system that has been overwhelmed and needs recovery conditions to restore its functioning.
For a comprehensive understanding of autism regression and what the neuroscience says about recovery, the post on autism regression covers everything parents need to know.
FAQs
Is autism a neurological disorder?
Autism is neurological in origin but whether it is accurately called a disorder depends on the framework used. It involves genuine brain differences that create real challenges alongside genuine strengths.
Is autism caused by brain damage?
No. Autism results from differences in brain development, not from damage. The autistic brain is differently organized, not damaged.
Is autism a mental illness?
No. Autism is a neurodevelopmental condition present from birth. Mental illnesses represent changes from a previous baseline. Autism is a fundamental aspect of how the brain is organized from the start.
Can autism be seen on a brain scan?
Not through standard clinical brain scans. Research using specialized imaging has identified consistent differences in autistic brains but these are not visible on routine clinical MRI or CT scans.
Is autism genetic?
Yes. Research suggests genetic factors account for around 80 percent of autism risk though the genetics are complex and involve many variants rather than a single gene.
Do vaccines cause autism? No. Decades of large scale research involving millions of children across multiple countries has consistently found no link between vaccines and autism.
Final Thoughts
Is autism a neurological disorder? The most accurate answer is that autism is a neurological difference whose impact on a person's life is shaped by both their neurology and the environment they are trying to function within.
The neurology is real. The differences in brain structure, connectivity, sensory processing, and information processing are measurable and consistent. The challenges those differences create in a world designed for neurotypical brains are also real.
But those challenges are not the whole story. The same neurological profile that makes some aspects of life harder also produces genuine and valuable strengths. The same brain that processes sensory information more intensely also notices things others miss. The same connectivity patterns that make social intuition more effortful also produce extraordinary depth of focus and pattern recognition.
The evidence, and the voices of autistic people themselves, consistently point toward flourishing as the better goal. And flourishing starts with understanding your own neurology accurately, compassionately, and completely.
References:
Cleveland Clinic. Neurological Disorders [Internet]. Last updated July 2024. https://my.clevelandclinic.org/health/diseases/neurological-disorders
Hernandez LM, Rudie JD, Green SA, Bookheimer S, Dapretto M. Neural Signatures of Autism Spectrum Disorders: Insights into Brain Network Dynamics. Neuropsychopharmacology. 2015 Jan;40(1):171-89. https://pmc.ncbi.nlm.nih.gov/articles/PMC4262896/
Patil O, Kaple M. Sensory Processing Differences in Individuals With Autism Spectrum Disorder: A Narrative Review of Underlying Mechanisms and Sensory-Based Interventions. Cureus. 2023 Oct 31;15(10):e48020. https://pmc.ncbi.nlm.nih.gov/articles/PMC10687592/
Chan MMY, Han YMY. Differential Mirror Neuron System (MNS) Activation During Action Observation With and Without Social-Emotional Components in Autism: A Meta-Analysis of Neuroimaging Studies. Mol Autism. 2020 Sep 29;11:72. https://link.springer.com/article/10.1186/s13229-020-00374-x
Kern JK, Geier DA, Sykes LK, Geier MR. Relevance of Neuroinflammation and Encephalitis in Autism. Front Cell Neurosci. 2016 Jan 19;9:519. https://pmc.ncbi.nlm.nih.gov/articles/PMC4717322/
What Is Pathological Demand Avoidance in Autism? A Complete Guide
Pathological demand avoidance in autism is one of the most misunderstood and underdiagnosed presentations on the autism spectrum. If you are a parent watching your child melt down over the simplest request, or an autistic adult who has spent years wondering why ordinary expectations feel physically impossible to meet, pathological demand avoidance in autism may be the framework that finally makes sense of what you have been experiencing.
This post covers everything you need to know about pathological demand avoidance in autism, from what it actually is, to how it presents, how it is identified, and what actually helps.
Table of Contents
What Is Pathological Demand Avoidance in Autism
Where the Term Comes From
How Pathological Demand Avoidance in Autism Differs From Typical Autism Presentations
Signs of Pathological Demand Avoidance in Autism in Children
Signs of Pathological Demand Avoidance in Autism in Adults
What Drives Pathological Demand Avoidance in Autism
How Pathological Demand Avoidance in Autism Is Identified
What Does Not Work and Why
What Actually Helps With Pathological Demand Avoidance in Autism
Pathological Demand Avoidance in Autism at School
How This Connects to Profound Autism and Autism Levels
The Role of Coaching and Support
FAQs
Final Thoughts
What Is Pathological Demand Avoidance in Autism
Pathological demand avoidance in autism is a profile of autism characterized by an extreme and pervasive drive to avoid everyday demands and expectations. The avoidance is not willful defiance. It is not laziness. It is not a parenting problem. It is an anxiety-driven neurological response to perceived loss of control and autonomy.
People with pathological demand avoidance in autism experience ordinary demands, getting dressed, eating breakfast, answering a question, going to school, as genuine threats to their sense of safety and autonomy. Their nervous system responds to these demands the way most people's nervous systems respond to actual danger. The fight, flight, or freeze response activates. And from that activated state, compliance feels neurologically impossible rather than simply undesirable.
Understanding pathological demand avoidance in autism starts with understanding that the word pathological here does not mean the person is broken or disordered in a moral sense. It means the demand avoidance is pervasive enough to significantly affect daily functioning across all environments. It is descriptive, not judgmental.
Where the Term Comes From
The term pathological demand avoidance in autism was first introduced by British psychologist Elizabeth Newson in the 1980s following her clinical observations of a group of children who did not fit neatly into existing autism diagnostic categories but shared a distinctive profile of extreme demand avoidance, surface sociability masking significant social difficulties, and a strong need to control their environment and the people in it.
Newson proposed pathological demand avoidance as a separate profile within the autism spectrum rather than a separate condition entirely. Her work has been built upon by researchers and clinicians in the UK, where pathological demand avoidance in autism is more widely recognized than in the United States.
It is worth noting that pathological demand avoidance in autism is not currently in the DSM-5, the diagnostic manual used in the US. This means it is not a formal diagnosis American clinicians can give. However, awareness of pathological demand avoidance in autism is growing in the US clinical community, and many clinicians are becoming more familiar with the profile even if they cannot formally diagnose it under that name.
How Pathological Demand Avoidance in Autism Differs From Typical Autism Presentations
Pathological demand avoidance in autism shares core features with other autism presentations but differs in several important ways that affect how support needs to be delivered.
Similarities with other autism presentations:
Social communication differences
Sensory sensitivities
Need for predictability and routine
Anxiety as a significant co-occurring feature
Difficulty with transitions
What makes pathological demand avoidance in autism distinct:
The demand avoidance is the central and most impairing feature, more so than social communication differences
People with pathological demand avoidance in autism often have better surface social skills than many autistic people, making the profile harder to spot
The avoidance strategies are highly varied, creative, and often socially manipulative in appearance, including distraction, negotiation, physical incapacity, and fantasy
Standard autism interventions, particularly those based on structure, compliance, and reward systems, often make pathological demand avoidance in autism worse rather than better
The anxiety driving pathological demand avoidance in autism is specifically triggered by demands and perceived loss of autonomy, not just by sensory or social overload
This distinction matters enormously for support. An autistic child without the pathological demand avoidance in autism profile may respond well to structured routines and clear expectations. A child with pathological demand avoidance in autism may become significantly more dysregulated by the same approach.
Signs of Pathological Demand Avoidance in Autism in Children
Recognizing pathological demand avoidance in autism in children is the first step toward getting them the right support. Here is what it commonly looks like:
Demand avoidance patterns:
Refusing or avoiding everyday tasks even ones the child enjoys or has done willingly before
Using creative strategies to avoid demands including distraction, negotiation, delay, and fantasy
Appearing not to hear instructions or suddenly becoming physically incapable
Intense resistance that escalates rapidly when pressure is applied
Control and autonomy:
Extreme need to be in control of their environment, activities, and interactions
Difficulty tolerating other people making decisions that affect them
May attempt to control others including parents, teachers, and peers
Strong reaction to perceived unfairness or being told what to do
Social presentation:
Often more socially aware and socially skilled on the surface than many autistic children
Can appear charming and engaging in low demand situations
Social difficulties become more visible under pressure or when demands are made
May use social skills strategically to avoid demands
Emotional regulation:
Extreme and rapid mood changes particularly in response to demands
Meltdowns that seem disproportionate to the triggering situation
High levels of anxiety that may not always be visible until a threshold is crossed
Difficulty recovering from dysregulation
Identity and fantasy:
Strong engagement with fantasy and role play sometimes used as a demand avoidance strategy
May inhabit characters or personas as a way of managing anxiety
Sense of identity can be fluid and variable
Signs of Pathological Demand Avoidance in Autism in Adults
Pathological demand avoidance in autism in adults often looks different from the childhood presentation because adults have developed more sophisticated strategies for managing their demand avoidance, often at significant personal cost.
Common presentations in adults:
Chronic difficulty maintaining employment because workplace demands trigger overwhelming anxiety
History of burnout from sustained effort to comply with demands over time
Difficulty with relationships because the implicit demands of intimacy and partnership feel overwhelming
Procrastination that goes far beyond typical avoidance and significantly affects daily functioning
Physical symptoms that emerge when demand load becomes too high, including fatigue, pain, and illness
Intense relief when demands are removed and intense dread when they return
A history of being told they are capable of more than they produce, creating significant shame
Many autistic adults who eventually learn about pathological demand avoidance in autism describe it as the first framework that explains a lifetime of experiences that nothing else adequately captured.
What Drives Pathological Demand Avoidance in Autism
Understanding what is actually happening neurologically in pathological demand avoidance in autism helps both parents and autistic individuals approach it with more compassion and more effective strategies.
The core driver of pathological demand avoidance in autism is anxiety, specifically anxiety about loss of autonomy and control. When a demand is made, the nervous system of a person with pathological demand avoidance in autism interprets it as a threat. Not a mild inconvenience or a minor frustration but a genuine threat that triggers the survival response.
From inside that threat response, compliance is not a choice that is being refused. It is a response that is neurologically unavailable. The brain is in survival mode. Survival mode and compliance are incompatible states.
This is why punishment, pressure, and reward-based systems so often fail with pathological demand avoidance in autism. They increase the demand load and therefore increase the anxiety, which makes the avoidance more extreme rather than less. The person is not being manipulative or oppositional. They are dysregulated.
What reduces the demand avoidance is reducing the anxiety. And what reduces the anxiety is increasing the sense of autonomy, safety, and control.
PDA in Autism
How Pathological Demand Avoidance in Autism Is Identified
Because pathological demand avoidance in autism is not in the DSM-5, getting it formally recognized in the US requires working with a clinician who is familiar with the profile.
Steps toward identification:
Seek assessment from a clinician who has specific experience with autism and who is familiar with pathological demand avoidance in autism as a profile
Request a comprehensive assessment that goes beyond the standard autism diagnostic tools to include detailed developmental history and behavioral observation
Use the Extreme Demand Avoidance Questionnaire, known as the EDA-Q, which is a validated tool developed specifically to assess the pathological demand avoidance in autism profile
Document specific examples of demand avoidance across different settings, home, school, community, to show the pervasive nature of the profile
Connect with clinicians and researchers in the UK where pathological demand avoidance in autism is more widely recognized and more clinical guidance is available
The Role of Coaching and Support
Living with pathological demand avoidance in autism, whether as the person who has it or as their parent or caregiver, is genuinely demanding in ways that most people around you will not fully understand.
For autistic adults with pathological demand avoidance in autism, the shame and confusion that comes from a lifetime of being told you are capable of more than you produce is one of the most significant things to work through. Understanding that the avoidance is neurologically driven rather than a character flaw is often the beginning of a profound shift in self-perception.
For parents, the grief and exhaustion of navigating a profile that most systems are not designed for, and that most professionals do not understand, is real and accumulating.
Both of these experiences deserve skilled, informed support.
Sonia's socio-emotional coaching works specifically with neurodivergent individuals on navigating the social and emotional landscape that pathological demand avoidance in autism creates, including how to communicate needs, build relationships that accommodate the profile, and develop strategies that work with the nervous system rather than against it.
What Does Not Work and Why
This section is important because many families with a child showing pathological demand avoidance in autism spend years trying approaches that make things worse before finding ones that help.
Approaches that typically worsen pathological demand avoidance in autism:
Strict behavioral programs based on compliance, reward, and consequence
Increasing structure and routine in response to avoidance
Applying more pressure when demands are refused
Using token economies or sticker charts that make demands more explicit
Issuing ultimatums or consequences for non-compliance
Trying to out-wait or outlast the avoidance
All of these approaches increase the sense of external control and therefore increase the anxiety driving the pathological demand avoidance in autism. They may produce short-term compliance in some children but they almost always increase the overall demand avoidance over time and significantly increase the risk of autistic burnout.
Also, reading books on Autism especially a lived experience is a way to navigation easier.
What Actually Helps With Pathological Demand Avoidance in Autism
The approaches that genuinely help with pathological demand avoidance in autism share a common thread: they reduce the perception of external demand and increase the sense of autonomy and collaboration.
At home:
Frame requests as choices rather than demands wherever possible
Reduce the number of direct demands in a day to the minimum necessary
Use indirect language, wondering out loud rather than instructing
Offer genuine choices about how and when tasks get done rather than whether they get done
Build relationship and trust as the foundation rather than compliance
Allow the child to lead activities regularly so they experience genuine control
Use humor, play, and indirection to reduce the felt demand of necessary tasks
Reduce the overall anxiety load by creating a low demand environment during recovery periods
What this looks like in practice:
Instead of: get your shoes on, we are leaving in five minutes. Try: I wonder if anyone around here has shoes that need to go on before we head out.
Instead of: you need to eat your dinner. Try: dinner is on the table whenever you are ready. What would you like to start with?
The goal is not to remove all demands from life. It is to reduce the experience of external imposition enough that the nervous system can stay regulated enough to participate.
Pathological Demand Avoidance in Autism at School
School is often the environment where pathological demand avoidance in autism is most visible and most challenging because school is fundamentally a high demand environment.
What schools need to understand about pathological demand avoidance in autism:
Standard behavior management approaches are likely to make things significantly worse
Reducing demands and increasing autonomy is not rewarding bad behavior, it is meeting a genuine neurological need
The child is not being defiant. They are dysregulated
Flexibility, relationship-based approaches, and genuine collaboration produce better outcomes than structure and compliance
What to advocate for in an IEP for a child with pathological demand avoidance in autism:
A low demand curriculum delivery approach
Flexibility around when and how tasks are completed
Genuine choice and agency built into the school day
A trusted key adult who can support regulation
Reduced whole-class participation requirements
A quiet withdrawal space available on demand
Staff trained specifically in pathological demand avoidance in autism approaches
FAQs
Is pathological demand avoidance in autism an official diagnosis in the US?
No. It is not in the DSM-5 but awareness among US clinicians is growing.
Is pathological demand avoidance in autism the same as oppositional defiant disorder?
No. ODD is behaviorally driven while pathological demand avoidance in autism is anxiety-driven and neurological in origin.
Can girls have pathological demand avoidance in autism?
Yes. Pathological demand avoidance in autism appears to affect girls at higher rates than other autism profiles and is frequently missed or misdiagnosed.
Does pathological demand avoidance in autism get better with age? With the right support and environment it can become more manageable but the underlying neurological profile does not disappear.
Should I tell my child's school about pathological demand avoidance in autism? Yes. Understanding the profile helps schools implement the right approaches and avoid the ones that make things worse.
Final Thoughts
Pathological demand avoidance in autism is not a behavior problem. It is not a discipline failure. It is not something that more consistency or firmer boundaries will fix.
It is a neurological profile in which the experience of demands triggers a genuine threat response that makes compliance neurologically unavailable rather than simply undesirable. Understanding pathological demand avoidance in autism at that level changes everything about how you respond to it, whether you are the person living with it or the parent, teacher, or clinician trying to support someone who is.
The right support for pathological demand avoidance in autism looks different from standard autism support. It prioritizes autonomy over compliance, relationship over structure, and nervous system regulation over behavioral management. When those conditions are in place, people with pathological demand avoidance in autism can and do thrive.
They just need the world to stop treating their neurology as a problem to be overcome and start treating it as a difference to be understood.
Listen to the On the Spectrum podcast with Sonia here for more honest, informed conversations about neurodivergent profiles, mental health, and what genuine support looks like.
References:
Wikipedia. Elizabeth Newson [Internet]. Last edited 2024. https://en.wikipedia.org/wiki/Elizabeth_Newson
Cleveland Clinic. DSM-5: What It Is & What It Diagnoses [Internet]. Last updated October 14, 2022. https://my.clevelandclinic.org/health/articles/24291-diagnostic-and-statistical-manual-dsm-5
Single Parenting an Autistic Child: Finding Support
There is a particular kind of exhaustion that single parents of autistic children know. It is not just the physical tiredness of doing everything yourself. It is the weight of being the only one who shows up to every appointment, fights every battle, fills out every form, absorbs every meltdown, and then gets up the next morning and does it all over again.
There is no one to hand it off to at the end of a hard day. No one to sit across the dinner table and share the worry with. No one who loves your child the way you do and understands what this life actually costs.
And yet, somehow, single parents of autistic children do it. Not perfectly. Not without breaking sometimes. But they do it, with a level of love and determination that is genuinely extraordinary.
This post is written for those parents. Not to tell you what you already know about how hard this is, but to give you something practical. Real strategies, real resources, and an honest conversation about finding support when the default assumption of the system is that there are two of you.
Table of Contents
The Unique Challenges Single Autism Parents Face
Give Yourself Permission to Need Help
Building Your Village From Scratch
Navigating Schools and Appointments Alone
Managing the Financial Pressure
Taking Care of Your Own Mental Health
How to Talk to Your Child About Your Family Structure
Finding Your Community Online and Offline
When You Need More Than Information
Final Thoughts
The Unique Challenges Single Autism Parents Face
Two parent families navigating autism have their own significant challenges. But single parenting adds layers that are worth naming honestly, because pretending they do not exist does not help anyone.
There is no backup
When your child has a three hour meltdown on a Tuesday night before a school meeting Wednesday morning, there is no one to take over while you recover. You absorb it and you keep going.
Every decision lands on you
Therapy choices, school placements, medication decisions, financial trade-offs. The weight of getting it right falls entirely on one set of shoulders.
Appointments multiply the problem
Autistic children often have multiple therapy appointments, school meetings, medical visits, and assessment reviews every month. Attending all of them while maintaining employment is a logistical challenge that two parent families split. Single parents carry it alone.
The emotional load has nowhere to go
Parenting an autistic child brings up complex emotions. Grief, guilt, fierce love, fear about the future, pride at every breakthrough. Without a partner to process with, those emotions can build up quietly until they become something harder to manage.
Self care feels impossible
When you are the only caregiver, taking time for yourself feels selfish at best and logistically impossible at worst. But the absence of self care is exactly what leads to the kind of burnout that makes everything harder.
None of this is said to overwhelm. It is said because the first step to finding support is being honest about what you actually need it for.

Give Yourself Permission to Need Help
This sounds simple. It is not.
Many single parents of autistic children carry a quiet shame about needing support. A sense that asking for help is an admission that they are not enough. That a good parent would manage. That the struggles they feel are a sign of failure rather than a completely reasonable response to an objectively hard situation.
That story is not true. And it is worth saying clearly.
Needing help is not a character flaw. It is a logical response to carrying more than one person was designed to carry alone. The parents who build the best lives for their autistic children are not the ones who white-knuckle it in isolation. They are the ones who are honest about their limits and strategic about getting support.
Giving yourself permission to need help is not the end of something. It is the beginning of building something better.
Building Your Village From Scratch
The phrase "it takes a village" gets thrown around a lot. For single parents of autistic children, building that village is not a nice-to-have. It is a survival strategy.
The village looks different for everyone. Here is how to start building one even when it feels like there is nothing there yet:
Start with who already exists
Family members, friends, neighbours, people from your faith community or social circle. Not everyone will understand autism. Not everyone will show up the way you need. But some will, if you ask directly and specifically rather than hoping they will figure out what you need on their own.
Be specific when you ask for help
Saying "I am struggling" often results in sympathetic words and no action. Saying "Could you pick my child up from school on Thursdays so I can make it to their therapy appointment?" gives someone a concrete, manageable way to show up.
Look for respite care options
Many countries and states have respite care programmes specifically for families of children with disabilities. Respite care provides temporary relief for caregivers, giving you scheduled time away from caregiving responsibilities. It is not abandonment. It is maintenance.
Connect with other single autism parents
There is a particular kind of understanding that only comes from someone who is living the same life. Other single parents of autistic children are not just a source of emotional support. They are a practical resource, people who know which services actually work, which professionals to avoid, and how to navigate the system with one set of hands.
Navigating Schools and Appointments Alone
School meetings and therapy appointments are where single parents most acutely feel the absence of a second person. Here is how to navigate them as effectively as possible on your own:
Bring an advocate to IEP meetings
Parent Training and Information Centers, available in every US state, provide free advocacy support to families. Having a knowledgeable advocate in the room means you are not alone at the table even when you are literally the only family member there.
Record meetings where permitted
Check the rules in your area, but in many places you are allowed to record school meetings. Having a record means you do not have to rely solely on your memory when you are processing a lot of information under pressure.
Ask for written summaries
After any significant appointment or meeting, request a written summary of what was discussed and agreed. This protects you when verbal commitments are later forgotten or disputed.
Batch appointments where possible
If your child sees multiple therapists or specialists, ask whether any of them can coordinate their scheduling. Even reducing the number of separate trips per week by one or two makes a meaningful difference to your capacity.
Use telehealth wherever available
Online therapy and appointments remove travel time entirely and allow you to be present without the logistical challenge of getting to a physical location. For single parents, this is not a convenience. It is often the difference between accessing support and not accessing it at all.
For a deeper look at what autism awareness vs autism acceptance means in practice and how to advocate effectively within systems that were not designed with your family in mind, that post covers the broader context every autism parent needs.
Managing the Financial Pressure
Single parenting is expensive. Single parenting an autistic child, with therapy costs, specialist equipment, additional childcare needs, and potentially reduced working hours to manage appointments, adds significant financial pressure to an already stretched budget.
Some practical steps that help:
Know what you are entitled to
Many families do not claim all the financial support available to them simply because they do not know it exists. Depending on where you live, this might include disability living allowance, carer's allowance, supplemental security income, Medicaid waivers, or local authority support funds. Research what is available in your specific location and apply for everything you qualify for.
Ask about sliding scale fees
Many therapists and coaches offer sliding scale pricing for families with financial constraints. It is always worth asking directly rather than assuming a service is out of reach.
Look into charitable grants
Several autism charities and foundations offer grants to families for therapy costs, specialist equipment, and other needs. These grants are underused because families do not know they exist. A quick search for autism family grants in your country or state is worth doing.
Connect with a financial advisor who understands disability
Some financial advisors specialise in working with families of children with disabilities and can help you navigate benefits, plan for your child's future, and make the most of the resources available to you.
Taking Care of Your Own Mental Health
This section is not optional. It is the most important one on this list.
Caregiver burnout does not announce itself dramatically. It creeps in quietly. It looks like chronic exhaustion that sleep does not fix. Emotional numbness. A growing inability to feel joy even in the moments that used to bring it. Resentment that frightens you because you love your child fiercely and the resentment feels like a betrayal of that love.
It is not a betrayal. It is a warning signal. And it deserves to be taken seriously.
Some things that genuinely help:
Therapy or coaching for yourself
Not for your child. For you. Single parents of autistic children carry enormous emotional weight and having a regular space to process that weight with someone trained to help is not a luxury. It is maintenance.
Scheduled time that belongs to you
Even thirty minutes a week that is entirely yours, a walk, a bath, a phone call with a friend, something that has nothing to do with caregiving. It sounds small. It adds up.
Honest conversations with your support network
The people around you cannot help with what they do not know about. Being willing to say "I am not okay right now" to someone who can respond is one of the bravest and most practical things a single parent can do.
The podcast is a space built for exactly the moments when you need to hear from someone who understands what this life actually looks like. Real conversations about the emotional reality of the autism parenting journey, including the parts that do not make it onto the highlight reel.
Listen to the podcast here and find the honest conversation you have been looking for.

How to Talk to Your Child About Your Family Structure
Autistic children often have a deep need for clear, honest, consistent information about their world. Uncertainty and vagueness are frequently more distressing than difficult truths delivered with love and clarity.
Some guidance for talking to your autistic child about your family structure:
Use clear, direct language
Autistic children tend to be literal thinkers. Metaphors and vague reassurances can create more confusion than comfort. Simple, honest, age-appropriate explanations work better.
Answer the questions they actually ask
Rather than pre-emptively delivering a full explanation, follow your child's lead. Answer what they ask, check for understanding, and make space for more questions as they come.
Normalise your family structure without over-explaining
Many family structures exist. Yours is one of them. Communicating that your family is complete and valid, rather than treating it as a deficit to be explained away, gives your child a healthier framework for understanding their own life.
Be consistent
Autistic children often return to the same questions repeatedly, not because they forgot the answer but because consistency and repetition are part of how they process and integrate information. Answer the same question with the same calm, clear answer as many times as it is asked.
Finding Your Community Online and Offline
Isolation is one of the most damaging things about single parenting an autistic child. And community, even imperfect community, is one of the most protective.
Some of the best places to find it:
Online single parent autism groups
Facebook groups, Reddit communities, and dedicated forums for single parents of autistic children exist and are genuinely active. These spaces offer something that is hard to find elsewhere: people who know exactly what your Tuesday night felt like.
Local autism family groups
Many areas have local autism family support groups that meet regularly. Being in a room with other autism parents, even those in two parent families, offers a level of understanding that friends and family outside the autism world often cannot.
Autism charity events and workshops
Many autism charities run events, workshops, and training sessions for families. These are practical, but they are also places where community forms naturally around shared experience.
School communities
Other parents in your child's school, particularly in special education settings, can become some of your most important relationships. They are navigating similar systems, facing similar challenges, and often willing to share information, support, and occasionally childcare.
The best selling autism books recommended for autism families include powerful accounts from parents and advocates who have navigated this road and documented what they learned along the way. Reading them will not solve everything, but it will remind you that you are not the first person to be standing where you are standing, and that people have found their footing from exactly this place.
When You Need More Than Information
There is a point in the single autism parent journey where information stops being what is needed. Where what is actually needed is a real conversation with someone who understands both the autism world and the emotional landscape of trying to navigate it alone.
That is where coaching makes a difference that no blog post can replicate.
Sonia Chand is a licensed psychotherapist offering specialised online coaching for parents and individuals navigating the autism journey. Two services are particularly relevant for single parents:
Socio-Emotional Coaching helps you develop the practical tools to navigate the complex social and institutional interactions that single autism parenting demands. IEP meetings, difficult conversations with family members who do not understand, advocating for your child in systems that push back. Coaching builds the skills and the confidence to show up in those moments effectively, even when you are showing up alone.
Self-Esteem Coaching works on something deeper. The chronic self-doubt that comes from carrying this much alone. The voice that tells you you are not doing enough, not getting it right, not enough full stop. Self-esteem coaching challenges that narrative directly and rebuilds the foundation of self-worth that makes every part of this journey more sustainable.
Both services are delivered entirely online, which means no commute, no childcare to arrange, and no barrier between you and the support you need.
Book a socio-emotional/self-esteem coaching session with Sonia here and build the tools to navigate this journey with more confidence and less isolation.
Final Thoughts
Single parenting an autistic child is one of the hardest things a person can do. That is not an exaggeration and it is not said to be dramatic. It is simply true.
But it is also true that the single parents who navigate this journey well are not superhuman. They are not doing it perfectly. They are doing it by being honest about what they need, strategic about finding support, and willing to ask for help even when everything in them wants to insist they are fine.
You are allowed to not be fine. You are allowed to need support. You are allowed to build a life that works for both you and your child, not just your child at the complete expense of yourself.
Your child needs many things. But one of the things they need most is a parent who is still standing. Who has not burned out completely. Who has enough left to be present, curious, and connected.
Taking care of yourself is not separate from taking care of your child. It is part of the same thing.
You are not doing this alone, even when it feels that way. The community exists. The support exists. And you deserve to find it.

How to Find an Autism Specialist in Your Area: A Guide
Finding the right autism specialist feels straightforward until you actually try to do it. Then comes the waiting lists, the confusing job titles, the referrals that go nowhere, and the growing sense that the system was not designed with your family in mind.
The truth is, finding the right support for your autistic child takes time, patience, and knowing what to look for before you start. Most parents figure this out by trial and error. This post exists so you do not have to.
Whether your child was recently diagnosed or you are revisiting their support plan because something is not working, this guide walks through exactly how to find the right autism specialist, what each type of professional actually does, and what to do when the usual routes are not enough.
Table of Contents
Start With a Clear Picture of What Your Child Needs
Understanding the Different Types of Autism Specialists
How to Find Autism Specialists in the UK
How to Find Autism Specialists in the US
What to Look for When Choosing a Specialist
Questions to Ask Before You Commit
When Traditional Routes Are Not Enough: Coaching as a Support Option
Socio-Emotional and Self-Esteem Coaching With Sonia Chand
Final Thoughts
Start With a Clear Picture of What Your Child Needs
Before searching for a specialist, it helps to get specific about what you are actually looking for. Autism support is not one size fits all and the right specialist for one child may not be the right fit for another.
Start by asking yourself these questions:
What is my child struggling with most right now?
Is the main challenge communication, sensory processing, behaviour, emotional regulation, or social connection?
Has my child already been diagnosed or are we still in the assessment stage?
What has already been tried and what has not worked?
Am I looking for clinical therapy, practical coaching, school support, or a combination?
Writing down the answers before you start making calls or filling in referral forms will save you a significant amount of time. It will also help you communicate your child's needs clearly to professionals who are seeing them for the first time.
The more specific you can be about what support you need, the faster you will find the right person to provide it.

Understanding the Different Types of Autism Specialists
One of the most confusing parts of navigating autism support is the sheer number of professional titles. Here is a plain language breakdown of who does what:
Developmental Paediatrician
A medical doctor who specialises in child development. Often involved in the initial diagnosis and ongoing medical monitoring. Your first point of contact if you are still in the assessment stage.
Child Psychologist or Clinical Psychologist
Assesses and supports emotional, behavioural, and cognitive development. Can provide therapy for anxiety, emotional regulation, and mental health challenges that often accompany autism.
Speech and Language Therapist
Works on communication, both verbal and nonverbal, as well as the social use of language. Particularly important for children who are nonverbal, have limited speech, or struggle with conversation and social communication.
Occupational Therapist
Supports sensory processing, fine motor skills, and daily living tasks. Helps children manage sensory sensitivities and develop the practical skills needed for school and home life.
Behaviour Analyst or ABA Therapist
Specialises in Applied Behaviour Analysis, a structured approach to building skills and reducing challenging behaviours. This type of therapy is widely used but also debated within the autism community, so it is worth researching thoroughly before committing.
Educational Psychologist
Focuses specifically on learning and how to support a child in an educational setting. Often involved in the process of getting an Education, Health and Care Plan in the UK or an IEP in the US.
Autism Coach or Specialist Coach
Works outside the clinical framework to support individuals and families with practical strategies, emotional regulation, social skills, and confidence building. Particularly valuable when clinical waiting lists are long or when a child needs ongoing personalised support beyond what therapy sessions provide.
How to Find Autism Specialists in the US
In the US, the route to finding autism support depends on your child's age, your insurance, and your state. Here is where to start:
Talk to your paediatrician
Ask for a referral to a developmental paediatrician or a child neurologist who can conduct or coordinate a full autism evaluation.
Contact your state's early intervention programme
For children under three, early intervention services are available in every state and are free regardless of income. These services can include speech therapy, occupational therapy, and developmental support.
Request an evaluation through your school district
Under the Individuals with Disabilities Education Act, known as IDEA, every child has the right to a free and appropriate public education. Schools are required to evaluate children suspected of having a disability at no cost to parents.
Use the Autism Speaks Resource Guide
At autismspeaks.org to search for specialists, therapy providers, and support organisations by zip code. It is one of the most comprehensive directories available to US families.
Check your insurance coverage
Most states now require insurance plans to cover autism-related therapies including ABA, speech therapy, and occupational therapy. Contact your insurance provider directly to understand what is covered and how to access it.
What to Look for When Choosing a Specialist
Once you have a list of potential specialists, the next step is knowing how to evaluate them. Qualifications matter, but they are not the only thing that matters.
Look for someone who:
Has specific experience working with autistic children, not just general child development experience
Takes a neurodiversity affirming approach, meaning they support your child's differences rather than trying to eliminate them
Communicates clearly with parents and keeps you involved in the process
Listens to your child and adapts their approach based on what works
Has a clear framework for measuring progress that goes beyond surface level behaviour
Be cautious of anyone who:
Promises rapid results or guaranteed outcomes
Focuses exclusively on making your child appear more neurotypical
Dismisses your concerns or talks over your knowledge of your own child
Uses punishment-based approaches or relies on distress as a motivator
Trust your instincts. You know your child better than any specialist does. The right professional will make you feel like a partner in the process, not a bystander.
For a broader understanding of what genuinely supportive autism care looks like, the post on autism awareness vs autism acceptance explains why the approach a specialist takes matters just as much as their credentials.

Questions to ask
Questions to Ask Before You Commit
Before starting with any new specialist, ask these questions directly:
What is your specific experience with autistic children at my child's age and support level?
What approach do you use and why?
How do you involve parents in the process?
How do you measure progress and how often will we review it?
What does a typical session look like for a child like mine?
What happens if the approach is not working?
Are you familiar with the current thinking around neurodiversity and autistic identity?
The answers will tell you a great deal about whether this is someone who will genuinely support your child or simply go through the clinical motions.
When Traditional Routes Are Not Enough: Coaching as a Support Option
Clinical therapy is essential for many autistic children. But it does not cover everything. Therapy sessions are typically short, infrequent, and focused on specific clinical goals. What many autistic children and their families also need is ongoing, personalised support that addresses the everyday challenges that do not fit neatly into a therapy framework.
This is where coaching comes in.
Coaching sits alongside clinical support rather than replacing it. It is particularly valuable for:
Autistic children and young people who struggle with social interactions and do not know how to navigate friendships, group settings, or school dynamics
Children who have the language and cognitive ability to engage in conversation but lack the emotional tools to manage relationships and regulate their responses
Young people whose confidence has been eroded by years of feeling different, misunderstood, or left out
Families who need practical, personalised guidance to implement strategies at home that actually work for their specific child
The right coach does not work from a generic template. They meet the child where they are, build on their strengths, and give them tools they can use in real situations, not just in a therapy room.
Socio-Emotional and Self-Esteem Coaching With Sonia Chand
Sonia Chand is a licensed psychotherapist offering specialised coaching services designed specifically for neurodivergent individuals and the families who support them.
There are two core coaching services available:
Socio-Emotional Coaching
Many autistic children understand the world in deep and meaningful ways but struggle to navigate the social landscape around them. They find friendships confusing, group dynamics overwhelming, and social rules that seem obvious to others completely invisible to them.
Socio-emotional coaching addresses exactly this. Working directly with the individual, Sonia provides practical, personalized guidance on navigating social interactions, building meaningful connections, and developing the emotional literacy that helps autistic people understand and express what they are feeling. The goal is not to make an autistic person behave like a neurotypical one. The goal is to give them a genuine toolkit for the world they are actually living in.
Self-Esteem Coaching
Years of feeling different, being corrected, struggling in environments not designed for them, and watching peers move through the world with what looks like ease can take a serious toll on an autistic child's sense of self. By the time many autistic young people reach adolescence, their confidence has taken significant hits that no amount of academic achievement or therapy alone can fully address.
Self-esteem coaching works on the inside. It helps autistic individuals reconnect with their strengths, challenge the narratives they have built about themselves, and develop a stable, grounded sense of who they are regardless of how the world around them responds.
Both services are available for neurodivergent individuals and are delivered with the practical, empathetic approach that comes from being both a licensed psychotherapist and someone who has navigated the autism journey personally.
Book a socio-emotional or self-esteem coaching session with Sonia here and give your child the tools to truly thrive.
Final Thoughts
Finding the right autism specialist is rarely quick and rarely straightforward. The system in both the UK and the US was not built for ease of navigation, and the waiting times alone can feel demoralizing when your child needs support now.
But the right support exists. The right people are out there. And knowing what to look for, what questions to ask, and where to search puts you in a far stronger position than most parents have when they start this process.
Go in informed. Go in with a clear picture of your child's specific needs. And do not be afraid to keep looking until you find the professional who genuinely gets your child and works with you as a partner.
Your child deserves that. And so do you.

ABA Therapy, Occupational Therapy and Speech Therapy for Autism Explained
When a child is diagnosed with autism, the word therapy comes up almost immediately.
Sometimes it comes up before the diagnosis is even confirmed. And for most parents, it arrives alongside a wave of acronyms, referral letters, and waiting lists that can feel completely overwhelming.
ABA. OT. SALT. SLT. Each one is a different discipline. Each one has its own philosophy, its own approach, and its own body of research. And each one means something different depending on who you ask.
The goal of this post is simple. To cut through the noise and explain what each therapy actually is, what it does, what the research says, and how to decide what is right for your child.
Because the decision about therapy is one of the most important ones a parent will make after diagnosis. And it deserves more than a rushed recommendation in a fifteen minute appointment.
Table of Contents
Why Therapy Decisions Matter So Much
ABA Therapy Explained
The Honest Debate Around ABA
Occupational Therapy Explained
What OT Actually Looks Like in Practice
Speech and Language Therapy Explained
What SALT Actually Looks Like in Practice
How the Three Therapies Work Together
How to Decide What Your Child Needs
Questions to Ask Before Starting Any Therapy
Helpful Resources
Final Thoughts
Why Therapy Decisions Matter So Much
Therapy is not neutral.
Every therapy your child receives communicates something to them about who they are and what is expected of them. Some approaches communicate that your child is capable and worthy of support. Others, unintentionally, communicate that your child's natural way of being is wrong and needs to be corrected.
That distinction matters enormously.
According to the World Health Organization, the abilities and needs of autistic people vary and can evolve over time. What works for one child may not work for another. And what looks like progress in one setting may not reflect genuine wellbeing in another.
According to data from the Centers for Disease Control and Prevention, about 1 in 31 children aged 8 years has been identified with autism spectrum disorder. That is a significant number of families navigating these decisions, often without enough information and often under enormous time pressure.
The earlier the right support is in place the better the outcomes tend to be. But earlier is only better if it is also the right kind of support.
That is why understanding what each therapy actually involves before committing to it is so important.
If your child was recently diagnosed and you are still finding your footing, the post on newly diagnosed: what to do after your child gets an autism diagnosis covers the broader landscape of first steps and is worth reading alongside this one.
ABA Therapy
ABA Therapy Explained
Applied Behaviour Analysis, known as ABA, is one of the most widely recommended and most heavily funded autism therapies in the world.
At its core, ABA is a science of behaviour. It applies principles of learning theory to understand why behaviours occur and to teach new skills or reduce behaviours that interfere with learning and daily life.
ABA works through a system of antecedents, behaviours, and consequences. In simple terms: something happens before a behaviour, the behaviour occurs, and something happens after that either reinforces or discourages the behaviour happening again.
In practice, ABA programmes typically involve:
Breaking skills down into small, teachable steps
Using positive reinforcement to encourage desired behaviours
Repeated practice of skills across different settings
Data collection to track progress over time
Individualised programmes based on each child's specific goals
ABA is delivered in different formats. Intensive programmes can involve up to forty hours per week. Less intensive programmes may involve a few hours per week. It can be delivered one-to-one, in small groups, at home, at school, or in specialist centres.
According to Autism Speaks, ABA is considered an evidence-based best practice treatment by the US Surgeon General and the American Psychological Association.
The Honest Debate Around ABA
ABA is also one of the most controversial topics in the autism community and that debate deserves an honest hearing.
Many autistic adults who experienced intensive ABA as children have spoken publicly about its impact. Some describe it positively. Others describe it as harmful, reporting that it taught them to suppress their natural autistic responses at significant psychological cost.
The criticism centres on a few key concerns:
Early ABA focused heavily on eliminating autistic behaviours like stimming rather than building genuine skills
The pressure to comply and perform can teach autistic children that their natural responses are wrong
The intense focus on normalisation can contribute to masking and the long-term costs that come with it
Some children experience ABA as stressful and coercive even when it is not intended to be
It is important to note that ABA has evolved significantly. Modern, naturalistic ABA looks very different from the intensive discrete trial training of earlier decades. The best ABA practitioners today focus on building functional skills, following the child's lead, and prioritising the child's quality of life rather than the reduction of autistic traits.
The key questions to ask of any ABA programme are: what is the goal of this therapy and does that goal centre the child's wellbeing or the comfort of the people around them?
Doing autism differently, which the post on doing autism differently: how to stop managing autism and start understanding it explores in depth, means applying that same question to every therapy decision you make.
Dropped in a Maze by Sonia Chand navigates exactly these kinds of decisions honestly. The moments of doubt, the wrong turns, and the clarity that eventually comes.
Order your copy here and read what most therapy leaflets will never tell you.
Occupational Therapy
Occupational Therapy Explained
Occupational therapy, known as OT, focuses on helping people participate in the activities of daily life.
For autistic children, that scope is broad. OT addresses the skills needed to function in everyday environments, at home, at school, and in the community.
The word occupational does not refer only to work. In this context, occupation means any meaningful activity. For a child, that includes playing, learning, dressing, eating, writing, and navigating sensory environments.
Occupational therapists who work with autistic children are trained to assess and support:
Sensory processing differences
Fine motor skills like writing, cutting, and fastening buttons
Gross motor skills like coordination, balance, and physical confidence
Self-care skills like dressing, toileting, and eating
Visual perceptual skills needed for reading and spatial awareness
Emotional regulation through a sensory lens
Participation in school and social environments
OT is often the therapy that makes the most visible difference to daily family life because it directly addresses the practical challenges that show up every single day.
What OT Actually Looks Like in Practice
An occupational therapy session for an autistic child might look very different from what most people expect.
It often looks like play.
A skilled OT uses carefully designed activities to build the skills they are targeting. Swinging, climbing, and movement-based play might be addressing sensory regulation. Building with blocks might be developing fine motor control. An obstacle course might be working on coordination and body awareness.
The child experiences it as fun. The therapist is simultaneously assessing, building, and monitoring the skills underneath.
OT also involves the family directly. A good occupational therapist will teach parents and carers how to carry strategies into daily routines so that progress is not limited to the therapy room.
Sensory processing is one of the areas where OT makes the biggest difference for many autistic children. Understanding your child's sensory profile, whether they are over-responsive, under-responsive, or seeking in different sensory channels, changes how you set up their environment, how you respond to their behavior, and how much unnecessary stress gets removed from their daily life.
The post on 7 common early signs of autism in infants and toddlers covers some of the early sensory signs worth watching for and why they matter for future support planning.

Speech and Language Therapy
Speech and Language Therapy Explained
Speech and language therapy, known as SALT or SLT, addresses communication in its broadest sense.
For autistic children, communication support goes far beyond helping a child produce words. It covers the full range of how a person sends and receives messages, verbally and nonverbally.
Speech and language therapists who work with autistic children focus on:
Developing spoken language where it is delayed or absent
Supporting nonverbal communication including gesture, facial expression, and body language
Building social communication skills including conversation, turn-taking, and understanding context
Introducing and developing augmentative and alternative communication systems for children who are nonverbal or minimally verbal
Addressing the literal processing of language that can make idioms, sarcasm, and implied meaning confusing
Supporting narrative skills, the ability to tell a story, explain an event, or describe an experience
Speech therapy is relevant for autistic children across the spectrum. It is not only for children who do not speak. Many verbal autistic children have significant support needs around the social use of language that speech therapy directly addresses.
What SALT Actually Looks Like in Practice
Like OT, speech therapy sessions for young children are typically play-based.
A speech therapist might use toys, books, games, and structured activities to target specific communication goals. They might work on back-and-forth interaction through play. They might model language without demanding it. They might introduce communication symbols or devices for a child who is nonverbal.
The best speech therapy is built around the child's interests and communication style rather than a generic programme applied to all autistic children equally.
It also extends beyond the therapy room. Parents and carers are taught strategies to use at home, at mealtimes, during play, and throughout daily routines. Because communication develops in relationship and context, not just in weekly appointments.
For a detailed look at communication strategies for nonverbal and minimally verbal autistic children, the post on nonverbal autism communication strategies and support goes deep on AAC, PECS, sign language, and technology-based communication tools.
The podcast also covers speech and communication regularly, with honest conversations about what progress really looks like and how families can support it at home.
Listen to the podcast here and get practical, experience-based insight on communication support for autistic children.
How the Three Therapies Work Together
ABA, OT, and speech therapy are not competing approaches. For many autistic children, they work best in combination.
Here is how they complement each other:
ABA provides the behavioural framework and skill-building structure. It can be used to teach the specific skills that OT and speech therapy identify as goals.
OT addresses the sensory and motor foundations that underpin learning and participation. A child who is in sensory overload cannot engage with ABA or speech therapy effectively. OT creates the conditions in which other therapies can work.
Speech therapy builds the communication skills that connect everything. A child who can communicate their needs, express discomfort, and engage with others has a fundamentally different experience of every other therapy they receive.
The key is coordination. The best outcomes happen when therapists are communicating with each other and with the family, working toward shared goals rather than operating in silos.
How to Decide What Your Child Needs
Every autistic child is different. The right combination of therapies depends on your child's specific profile, not on a standard post-diagnosis checklist.
Some starting questions worth asking:
What are my child's most significant areas of need right now? Communication, sensory processing, motor skills, and behaviour all point toward different therapy priorities.
What are my child's strengths? Good therapy builds on strengths rather than only targeting deficits. A therapist who cannot identify your child's strengths quickly is worth questioning.
What does my child enjoy? Therapy is most effective when it is motivating. A child who is distressed in therapy sessions is not learning effectively regardless of the approach.
What can our family sustain? Therapy schedules can become consuming. A realistic, sustainable programme that the family can implement consistently is more valuable than an intensive programme that burns everyone out within six months.
What are the goals? Every therapy goal should be clearly stated, measurable, and centred on your child's quality of life. If a goal is about making your child appear more neurotypical rather than genuinely improving their wellbeing, that is worth interrogating.
Questions to Ask Before Starting Any Therapy
Before committing to any therapy programme, these questions are worth asking directly:
What specific goals will this therapy target for my child?
How will progress be measured and how often will it be reviewed?
What does a typical session look like?
How will you involve me as a parent in carrying strategies into daily life?
What is your approach to autistic identity and acceptance?
What happens if my child is distressed during sessions?
Do you have experience working with children at my child's level of support need?
Can you provide references or connect me with other families you have worked with?
A good therapist will welcome these questions. They will answer them clearly and directly. And they will treat you as a genuine partner in your child's support rather than someone to be managed alongside the child.
Final Thoughts
Therapy is a tool. Like any tool, its value depends entirely on how it is used and whether it is the right tool for the job.
ABA, occupational therapy, and speech therapy each have genuine evidence behind them. Each can make a meaningful difference in an autistic child's life when implemented well, by skilled practitioners, with clear goals, and with the child's wellbeing genuinely at the centre.
None of them are magic. None of them work the same way for every child. And none of them replace the most important thing of all, a family that understands their child deeply and advocates loudly for what they need.
That understanding is what Dropped in a Maze is built around. Not a guide to therapies but an honest account of navigating the whole landscape, the decisions, the doubts, and the moments when everything finally begins to make sense.
Order your copy of Dropped in a Maze here. Because the therapy decisions are just one part of a much bigger journey and you deserve support for all of it.

15 Reasons Why Being on the Autism Spectrum Is Awesome
For most of my life, the world told me that my autism was a problem to be solved. I was made to feel like I was too much, not enough, and everything in between. But somewhere along the way, I stopped believing that story.
I am an autistic psychotherapist, advocate, author, and ultra-marathoner. I wrote Dropped in a Maze: My Life On The Spectrum because I needed the world to hear a different kind of story about autism. Not the clinical one. Not the one written by people who have never lived it. The real one.
In the book, I share 26 reasons why being on the spectrum is something to be celebrated. Today I am sharing 15 of them with you. Because if nobody has told you lately, being autistic is not your weakness. It is one of your greatest strengths.
Table of Contents
Intro
15 Reasons Why Being on the Autism Spectrum Is Awesome
Conclusion
There Is So Much More in the Book
1. You Think of Things in Different Ways
You can put a unique perspective on ideas because Autism taught you to think differently. That perspective is not a flaw. It is something most people will never have access to, and it belongs entirely to you.
2. You Are Intelligent in the Things You Are Passionate About
Autism allows you to absorb information about the things you hyper-focus on at a depth that is extraordinary. That kind of knowledge is rare. Own it.
3. You Take Your Passions Seriously
You geek out on the things you love with immense pride, and you should. Not everyone has the ability to go that deep into something they care about. You do.
4. You Have a Unique Sense of Humor
You like to laugh at random things, and that humor is entirely your own. After all, laughter makes life fun, right?
5. You Are a Late Bloomer and That Is a Gift
You get excited by milestones in ways that other people may take for granted because they may have already surpassed them long ago. That excitement keeps a positive outlook on life alive in you. Do not underestimate how powerful that is.
6. You Are Capable and Equipped to Take On Life's Challenges
Autism taught you to be resilient and strong. That resilience was not handed to you. It was built through real experience, and it makes you genuinely capable of handling whatever life puts in front of you.
7. You Are Strong Mentally and Physically
Autism taught you to be both in order to keep affecting change and thrive in a world that is not always welcoming of neurodivergence. That strength is yours, and it shows.
8. You Are a Warrior
Autism taught you to fight for the life you deserve. Not once, not occasionally, but consistently, even when the world was not on your side. That warrior spirit is something to be proud of.
9. You Are Ambitious
Autism taught you that you can use your strengths and desires to attain the life you want. That ambition, grounded in self-knowledge, is more powerful than most people realize.
10. You Are Good at Helping People
Autism showed you the ugly side of humanity, and instead of hardening you, it taught you to rise above it and show people more love and kindness. That choice is what makes you exceptional at helping others.
11. You Have a Strong Ability to Empathize
Even when you may not always completely understand, Autism taught you that you needed to set an example so that people could learn to one day understand you. That effort is its own form of emotional leadership.
12. You Learned to Become Your Own Best Friend
Autism taught you that the most important person in your corner was yourself. That relationship is one of the most valuable ones you will ever have.
13. You Are Fiercely Loyal and Compassionate
Autism taught you well enough how it feels when people are not. That knowledge shaped who you chose to become, and the people you love feel the difference every single day.
14. You Learned to Embrace the Word Weird
Autism taught you that it is okay to be your unique self. Anything otherwise would be a disservice to yourself and to everything you offer the world.
15. You Learned to Use Your Challenges as Your Strengths
Autism showed you that turning challenges into strengths was a way to go forth and prosper. What the world called a limitation, you turned into your foundation.
If you found yourself nodding along to these 15 reasons, this is worth reading next: How to Stand Up for Yourself as an Autistic Person
Conclusion
Being on the spectrum is a layered experience. It is not just the challenges people read about in articles or hear about in passing conversations. It is also the resilience, the depth, the loyalty, the humor, and the fierce love you carry with you every single day.
The 15 reasons above are just a starting point. They are reminders that your brain is not broken. It is wired differently, and that difference has given you a set of qualities that the world genuinely needs. Your ability to think in ways others cannot, to feel things deeply, to persevere when most people would have stopped, and to turn pain into purpose are not small things. They are remarkable.
If you have ever been made to feel like autism was the reason you could not have the life you wanted, I want you to sit with these 15 reasons and read them again. Because autism is also the reason you are as strong as you are. It is the reason you do not give up. It is the reason you know the value of kindness in a way that people who have never struggled do not.
You are not behind. You are not broken. You are building something, and it is worth celebrating.
There Is So Much More in the Book
These 15 reasons are just a glimpse of what is inside Dropped in a Maze: My Life On The Spectrum. In the book, I share all 26, alongside the raw and honest story of what it has really meant to live on the spectrum, fight for a place in the world, and come out the other side knowing your worth.
If you are autistic, this book was written for you. If you love or support someone who is, this book will help you understand them in a way that nothing else can.
Purchase your copy of Dropped in a Maze here
If this post resonated with you, come and hear more. I talk about neurodivergence, mental health, self-advocacy, and life on the spectrum with the kind of honesty and depth you will not find everywhere.
Sonia Chand is an autistic psychotherapist, advocate, author, and ultra-marathoner. Her work is dedicated to changing the narrative around autism one story at a time. Visit her at soniakrishnachand.net.
Social Skills Autistic Adults Need
Most people learn basic social skills naturally throughout childhood—table manners, how to walk confidently, appropriate fidgeting management. But for autistic people, these skills often need to be explicitly taught. And by the time you reach adulthood without them, the gap becomes glaringly obvious.
The embarrassment of being in your mid-twenties and needing someone to teach you how to hold a fork properly, walk fluidly, or order appropriately at restaurants is profound.What's rarely discussed is how practical, specific coaching in these areas can transform your social experiences, when delivered constructively rather than judgmentally.
This is about the social skills autistic adults actually need, how constructive coaching differs from harmful criticism, and why learning these basics in your twenties (or thirties, or forties) isn't shameful—it's courageous.
Table of Contents
Skill #1: Table Manners and Eating Mechanics
Skill #2: Proper Posture and Fluid Movement
Skill #3: Managing Fidgeting and Stimming in Social Settings
Skill #4: Appropriate Food Choices and Healthy Eating Presentation
Skill #5: Personal Grooming and Appearance Details
Skill #6: Flexibility in Social Planning
Skill #7: Distinguishing Constructive Feedback From Harsh Judgment
The Difference Between Helpful Coaching and Harmful Criticism
Key Takeaways for Learning Social Skills as an Adult
Skill #1: Table Manners and Eating Mechanics
Why This Matters
According to the National Library of Medicine, motor planning difficulties are common in autistic people and can affect fine motor tasks like using utensils properly. When Kelly first observed me eating, she noticed several issues I was completely unaware of.
What I Needed to Learn
Eating pace: "The first thing is you need to eat slowly. Remember this rule: two bites, one sip of water, two bites, one sip of water."
Fork grip and mechanics: I was holding my fork incorrectly and using it like a spoon at times. The fork was hitting my teeth and making noise.
Proper utensil-to-mouth motion: Kelly demonstrated the correct way to bring food to my mouth and had me practice until I got it right.
Why This Is Important for Dating and Professional Life
As Kelly explained: "We are going to focus on eating because when you first start dating someone, that is what you are going to be doing."
First dates typically involve meals. Business meetings happen over lunch or dinner. Poor table manners create negative first impressions that can overshadow everything else about you.
The Embarrassment Factor
It felt profoundly embarrassing that someone in her mid-twenties needed to be taught table manners that others learn substantially younger. But the embarrassment of learning is temporary—the impact of not learning lasts forever.
How to Practice
Watch yourself eat in a mirror to see what others see
Practice the two-bite, one-sip rhythm until it becomes automatic
Record yourself eating to identify specific issues
Ask trusted people for honest feedback about your eating habits
If you missed signs of autism in your youth that could have led to earlier intervention in these skills, read our article on The Journey to Autism Diagnosis: 7 Signs You Might Have Missed in Young Adults for more context.
Skill #2: Proper Posture and Fluid Movement
The Walking Problem
Dr. Grey had previously noticed that my walk wasn't fluid motion. Kelly confirmed this after seeing me walk up stairs and around the mall.
I had a "funny gait" from early childhood—glimpses of memories of walking on my tiptoes, never being fully comfortable with my whole foot on the floor. People had called me out on my walk throughout my life, saying I walked "weird" or too fast, but nobody got into specifics until now.
What I Needed to Learn
Standing posture: Walk standing up straight with shoulders back
Heel-to-toe motion: Use the whole foot in fluid motion, not just toes or balls of feet
Pace and rhythm: Walk at a normal pace rather than rushing
Stair climbing form: Proper technique for going up and down stairs
Why This Matters
Body language communicates before you speak. How you carry yourself signals:
Confidence or insecurity
Comfort or awkwardness
Social awareness or obliviousness
An awkward gait or poor posture can make people uncomfortable around you without them consciously knowing why.
The Lifelong Impact
Poor motor skills don't just affect walking. They impact:
How you're perceived professionally
Whether people feel comfortable around you
First impressions in social and romantic situations
Your own confidence and self-image
How to Practice
Practice walking in front of a mirror to see your posture
Video yourself walking from different angles
Focus on one element at a time: first shoulders back, then heel-to-toe, then pace
Ask for feedback from people who will be honest and constructive
Skill #3: Managing Fidgeting and Stimming in Social Settings
The Hair-Playing Problem
Kelly noticed I played with my hair during meals. She taught me to keep my hands together on my lap when I felt the urge to fidget.
This remains a work in progress, as I have a tendency to fidget with my hair for sensory regulation.
The Balancing Act
For autistic people, stimming serves important regulatory functions. But in professional or dating contexts, obvious stimming can distract others or signal anxiety and discomfort.
Finding Middle Ground
The goal isn't to eliminate stimming entirely—it's to:
Develop less noticeable stims that still provide sensory input (hands on lap, subtle foot tapping)
Save more obvious stims for private moments (hair playing, hand flapping when alone)
Recognize when stimming is increasing and what triggers it (anxiety, overstimulation)
Communicate needs when necessary ("I need a moment to step away and regulate")
Practical Strategies
Identify your most common stims and when they occur
Practice replacement behaviors that are less noticeable
Use discrete fidget tools (smooth stones in pocket, textured jewelry)
Take strategic breaks to stim freely in private
For more on finding therapists and coaches who understand these balance between autistic needs and social expectations, read our article on 5 Signs You've Found the Right Therapist.
Skill #4: Appropriate Food Choices and Healthy Eating Presentation
The Appetizer Incident
During one dinner, Kelly noticed I ordered only an appetizer that wasn't nutritionally valuable. She taught me about ordering healthy foods when eating out.
Her reasoning: "Eating healthy shows people you care about yourself and take care of yourself."
Why This Matters
Food choices signal to others:
Whether you value your health
Your level of self-care
Whether you can make adult decisions
How you'll approach other life areas
The Broader Lesson
This wasn't about restriction or diet culture. It was about demonstrating self-care through choices that show you value yourself.
Ordering appropriately also includes:
Matching the formality of the setting (don't order appetizers only at a formal dinner)
Being adventurous without being inappropriate (don't order the messiest item on a first date)
Considering portion sizes (don't order so much you can't finish or so little you seem restrictive)
Reading the situation (casual lunch versus important business dinner)
How to Develop This Skill
Research menus ahead of time so you're not deciding under pressure
Observe what others order in similar settings
Ask trusted friends for feedback on your food choices
Practice ordering at different types of restaurants
Skill #5: Personal Grooming and Appearance Details
The Constructive Difference
Kelly never commented on my weight—a stark contrast to Dr. Grey's obsessive focus on thinness. Instead, she addressed specific, actionable grooming issues:
Hair appearing disheveled
Bra fit being incorrect
Needing to pay more attention to these aspects before leaving the house
Why This Approach Works
Constructive feedback on grooming:
Focuses on specific, fixable issues
Doesn't shame your body or natural appearance
Provides actionable steps
Addresses presentation, not inherent worth
Common Grooming Gaps for Autistic Adults
Many autistic adults struggle with:
Knowing when hair needs washing or styling
Understanding proper undergarment fit
Recognizing when clothes need replacing
Applying makeup appropriately (if choosing to wear it)
Maintaining consistent hygiene routines
How to Address These Gaps
Create checklists for daily grooming routines
Get professional fittings for undergarments
Ask trusted friends for honest appearance feedback
Set up systems (hair washing schedule, clothing replacement timeline)
Take photos to see how you actually look versus how you think you look
Skill #6: Flexibility in Social Planning
The Restaurant Change Incident
When Kelly set us to meet at a restaurant whose menu didn't appeal to me, I reluctantly asked if we could go somewhere else. She agreed, but her unhappiness showed.
Her response: "Don't do this again! What would've happened if you had done this on a date? Your date would've probably been pissed off and annoyed."
The Social Rule I Violated
Once plans are set, changing them is generally inappropriate unless there's a significant reason (allergies, dietary restrictions, genuine emergency).
Changing plans because you don't like the menu signals:
Inflexibility
Difficulty compromising
Prioritizing your preferences over others'
Poor planning (you should have checked the menu before agreeing)
The Competing Needs
My suspicion was that Kelly may have been bothered because she genuinely wanted to eat at the original restaurant. This highlights the complexity:
Sometimes what's labeled "teaching you social skills" is actually about the other person's preferences.
Learning Flexibility
For autistic people who struggle with food texture, routine, or unexpected changes:
Communicate dietary restrictions upfront: "I have sensory issues with certain foods. Can we choose a restaurant together?"
Review menus before agreeing to plans: Check that there's at least one item you can eat
Bring backup foods if necessary: Keep safe foods available for difficult situations
Practice tolerating imperfect situations: Not every meal needs to be ideal
Skill #7: Distinguishing Constructive Feedback From Harsh Judgment
Constructive Coaching (Kelly's Approach)
Kelly's feedback was:
Specific: "You're making noise with your fork hitting your teeth"
Actionable: "Here's how to hold your fork properly. Watch me, then follow."
Focused on teachable skills: Table manners, walking mechanics, grooming details
Free of body shaming: Never commented on weight, only on specific presentation issues
Harsh Judgment (Dr. Grey's Approach)
Dr. Grey's feedback was:
General and demoralizing: "Something isn't working if you've been going to the gym"
Focused on unchangeable aspects: Body size, facial attractiveness ratings
Lacking specific guidance: "Everything has to be perfect" without defining what that means
Undermining confidence: "Girls are just being nice when they compliment you"
The Breaking Point
Eventually, I had enough of Dr. Grey's weight obsession. When he continued his "serenade about how some of his clients wouldn't go out with women five pounds overweight," I finally pushed back:
"Don't you think it's possible that these clients who are fussing about women being five pounds overweight are just being shallow? Women can pick up on men who are shallow and will keep their distance."
Why This Distinction Matters
Constructive coaching:
Builds skills and confidence
Provides specific, actionable steps
Respects your inherent worth
Focuses on what you can control
Harsh judgment:
Tears down self-esteem
Creates impossible standards
Ties worth to appearance or others' opinions
Focuses on what you can't easily change
Ready to hear more about navigating the difference between helpful support and harmful criticism? Listen to the On the Spectrum Empowerment Stories podcast for real conversations about what actually helps autistic adults build genuine confidence.
Helpful Coaching and Harmful Criticism
The Difference Between Helpful Coaching and Harmful Criticism
What Made Kelly's Approach Effective
She focused on skills, not worth: Table manners and walking mechanics are learnable skills, not indicators of value as a person.
She demonstrated and practiced: "Watch me, then follow" is effective teaching methodology.
She acknowledged progress: Kelly noticed improvement and commented on it, reinforcing positive changes.
She explained the 'why': Understanding that first dates involve eating helps you prioritize learning table manners.
She addressed specific, fixable issues: Disheveled hair and poor bra fit are concrete problems with concrete solutions.
What Made Dr. Grey's Approach Harmful
He focused on unchangeable aspects: Body size, facial structure, inherent attractiveness.
He provided contradictory messages: Be thin, but also treat yourself to ice cream.
He reinforced perfectionism: "Everything has to be perfect" creates impossible standards.
He undermined confidence: Dismissing genuine compliments as "just being nice."
He projected his clients' shallowness: Treating five-pound weight concerns as legitimate rather than problematic.
The Key Question
After any coaching or feedback session, ask yourself:
Do I feel empowered with specific things I can practice and improve, or do I feel inadequate and hopeless about unchangeable aspects of myself?
If it's the latter, you're receiving harmful criticism, not helpful coaching.
Key Takeaways for Learning Social Skills as an Adult
It's Not Too Late to Learn
Being in your twenties, thirties, or beyond when you finally learn basic social skills doesn't mean you're broken. It means:
You didn't receive the explicit instruction autistic people need
You're brave enough to address gaps now
You're investing in your future social success
Many autistic adults have these same gaps. You're not alone.
Embarrassment Is Temporary, Impact Is Permanent
Yes, it's embarrassing to need table manners coaching as an adult. But:
The embarrassment of learning lasts weeks or months
The benefit of knowing these skills lasts your entire life
People won't remember you needed to learn; they'll just notice you have good manners now
Focus on Specific, Actionable Skills
Effective social skills coaching addresses:
Table manners and eating mechanics
Posture and movement
Grooming and presentation details
Social conventions and flexibility
Ineffective coaching focuses on:
Body size and weight
Inherent attractiveness
Impossible perfectionism
What others think of you
Find Coaches Who Build You Up
The right coach or therapist:
Provides specific, actionable feedback
Acknowledges your progress
Explains why skills matter
Respects your inherent worth
Focuses on what you can control
The wrong coach:
Makes you feel worse about yourself
Provides vague or contradictory advice
Focuses on unchangeable aspects
Ties your worth to others' shallow judgments
Progress Takes Practice
Kelly noticed improvement in my fork grip and eating pace after just a couple of sessions because I practiced the specific techniques she taught.
Social skills improve through:
Conscious practice of specific techniques
Immediate feedback on what's working
Repetition until skills become automatic
Patience with yourself during the learning process
For the complete story of learning these social skills as an adult—including every embarrassing moment, every breakthrough, and what actually worked versus what wasted my time—my book provides all the details you need.
Moving Forward
If you're an autistic adult who knows something is "off" about your social presentation but can't pinpoint what, you're not alone. Most autistic people need explicit coaching in skills neurotypical people absorb through observation.
The key is finding coaches and therapists who can provide that explicit guidance constructively, building your skills and confidence simultaneously.
Ready to learn the complete story of navigating social skills coaching, distinguishing helpful feedback from harmful criticism, and eventually developing genuine confidence? My book details every session with both Kelly and Dr. Grey, showing you exactly what works and what doesn't.

6 Ways Your Therapist May Be Harming You (Even If They Specialize in Autism)
Finding a therapist who specializes in autism feels like winning the lottery, especially after years of working with practitioners who don't understand your neurological differences. But specialization in autism doesn't automatically equal good therapy.
Sometimes the most harmful therapeutic relationships come from practitioners who understand autism intellectually but apply that knowledge in ways that reinforce shame, perfectionism, and self-hatred rather than building genuine self-worth.
This is about recognizing when autism-informed therapy crosses the line from helpful to harmful, and what to do when your therapist's advice is damaging your mental health instead of supporting it.
Table of Contents
Harmful Pattern #1: Obsessive Focus on Your Appearance and Weight
Harmful Pattern #2: Contradictory Messages That Keep You Confused
Harmful Pattern #3: Reinforcing That You Need to Be "Perfect"
Harmful Pattern #4: Judging People With Mental Health Struggles
Harmful Pattern #5: Discouraging Career Paths Based on Your Autism
Harmful Pattern #6: Telling You to Care What Everyone Thinks
What Healthy Autism-Informed Therapy Actually Looks Like
How to Protect Yourself From Harmful Therapy
Harmful Pattern #1: Obsessive Focus on Your Appearance and Weight
When Body Image Becomes Central to Treatment
One of Dr. Grey's frequent topics was my weight and appearance. Sessions would begin with questions like "So, you were never known as the heavy child?" followed by critiques of my eating habits, exercise routine, and overall appearance.
His advice included:
"Maybe you need to start eating more lean meat and protein-based foods"
"Hire a nutritionist to help you"
"Something isn't working if you have been going to the gym as often as you say"
When I mentioned girls complimenting my appearance: "They are just trying to be nice to you"
The Damaging Message
The culmination was this statement: "The reason I am telling you all this is that with your autism and mood disorder, everything has to be perfect. Thin girls get away with more."
This message communicated that:
Your neurological differences mean you're starting from a deficit
You must compensate for autism by achieving physical perfection
Other people's superficial judgments should dictate your self-worth
Being thin is a prerequisite for social acceptance
Why This Is Harmful
According to the National Eating Disorders Association, autistic people already have higher rates of eating disorders and body image issues. A therapist reinforcing that thinness equals worthiness can:
Trigger or exacerbate disordered eating
Create shame about natural body diversity
Tie self-worth to appearance rather than character
Add perfectionism on top of existing mental health struggles
What I Needed Instead
Therapeutic support should have addressed:
Using food emotionally as a coping mechanism
Building self-worth independent of appearance
Challenging societal beauty standards, not reinforcing them
Developing healthy relationship with body and food
For more on recognizing when therapeutic relationships have crossed into harmful territory, read our article on 5 Signs You've Found the Right Therapist (And 3 Red Flags You're With the Wrong One).
Contradictory Messages
Harmful Pattern #2: Contradictory Messages That Keep You Confused
The Ice Cream Paradox
Dr. Grey's messages often contradicted each other:
One session: "Because of your autism and mood disorder, everything has to be perfect. This means you need to be thin. People these days are obsessed with airbrushing, and I have clients who won't date a girl who is even five lbs overweight."
Another session: "On days you feel bad, you need to learn to go do something for yourself, such as go get an ice cream."
Why Contradictory Advice Harms
When therapeutic messages contradict each other:
You can never get it right. Whatever you do violates one piece of advice or another.
You lose trust in your judgment. If the expert keeps changing the rules, you stop trusting your own decisions.
You stay dependent on the therapist. Confusion keeps you coming back for clarity that never arrives.
You internalize the contradiction. The conflicting messages become your inner dialogue—"be perfect" versus "treat yourself" creates paralysis.
The Pattern Across Multiple Areas
The contradictions extended beyond food:
Be yourself / Change everything about yourself
Don't care what people think / Care deeply about what everyone thinks
Build self-worth / Your worth depends on others' judgments
Love yourself / You're not attractive enough as you are
What Consistent Therapeutic Messaging Looks Like
Effective therapy provides:
Clear, consistent principles you can rely on
Messages that align across different situations
Support for developing your own judgment
Acknowledgment when approaches need to shift, with explanation
For the complete story of my autistic journey through law school my book provides all the details, order your copy today.
Harmful Pattern #3: Reinforcing That You Need to Be "Perfect"
The Impossible Standard
Dr. Grey's recurring message: "Because of your autism and mood disorder, everything has to be perfect."
This extended to:
Physical appearance: Thin, fashionable, makeup done correctly
Social skills: Every interaction executed flawlessly
Body language: Walk correctly, posture perfect, no "weird" movements
Dating: Compensate for autism by achieving perfection in all areas
Why Perfectionism Is Toxic for Autistic People
Autistic people already tend toward:
All-or-nothing thinking
High standards for themselves
Difficulty with self-compassion
Shame about not meeting neurotypical expectations
A therapist reinforcing that you must be perfect to be acceptable amplifies these existing vulnerabilities.
The Impossible Equation
The message was clear: Autism + Mood Disorder = Need for Perfection to Compensate
This creates an impossible situation where:
Your neurological differences are framed as deficits
You must work harder than neurotypical people to be "acceptable"
Any imperfection confirms you're not trying hard enough
There's no room for being human, making mistakes, or having bad days
What I Started Teaching Myself Instead
During my deepest depression, I began practicing: "I am a sexy diva," repeatedly in front of the mirror. At first it felt weird, but it became a routine I loved.
When Dr. Grey dismissed this with "Guys don't see you like that," I responded: "I don't care what guys see me as. It's the opinion of myself that should count first, Dr. Grey."
Harmful Pattern #4: Judging People With Mental Health Struggles
The Stigmatizing Statement
During one session, Dr. Grey said: "The unfortunate truth is when people have any kind of psychiatric diagnosis, others don't like to be around that person. People step back."
He continued: "People want to be around someone who has sunshine in their hearts. People don't like to be around people who have all sorts of issues."
The Professional Betrayal
This statement from a psychotherapist—someone whose job is to support people with mental health struggles—was profoundly damaging.
It communicated:
Your mental health diagnosis makes you inherently undesirable
You should hide or minimize your struggles to be acceptable
People are right to avoid those with psychiatric diagnoses
Your worth is contingent on appearing "issue-free"
Why This Is Unethical
A mental health professional stigmatizing psychiatric diagnoses:
Violates the fundamental premise of therapeutic support
Reinforces societal stigma clients come to therapy to escape
Creates shame about seeking help or having diagnoses
Makes clients feel judged in what should be a safe space
The Question This Raises
As I noted at the time: "It made me wonder why someone like him was even a psychologist, but like in any profession, people can enter it for the wrong reasons."
When your therapist judges the very population they're supposed to serve, it reveals they're in the field for reasons other than genuine care and support.
If you're questioning whether your autism diagnosis was missed or misunderstood in your youth, read our article on The Journey to Autism Diagnosis: 7 Signs You Might Have Missed in Young Adults for more context.
Harmful Pattern #5: Discouraging Career Paths Based on Your Autism
The Limiting Beliefs
Despite my expressed desire to become a therapist and help others on the autism spectrum, Dr. Grey actively discouraged this path.
His reasoning:
Autism meant people wouldn't connect with me
I shouldn't be in mental health or trial law
I was better suited for financial advising where expertise mattered more than connection
The Deeper Issue
This advice revealed:
Limited vision of what autistic people can do: Assuming autism automatically disqualifies you from relationship-based work
Projection of his own biases: Perhaps his difficulty connecting with clients reflected his limitations, not autism's
Ignoring my strengths and passions: My heart was suited to helping others heal and feel understood
Reinforcing family pressure: Aligned with parents who wanted me to stay in law school rather than pursuing what called to me
What I Actually Knew
My desire to work in mental health came from authentic experience: "I wanted to be that person for someone else in ways I wish I had that someone for myself."
This is often the deepest calling—helping others through struggles you've survived yourself.
The Career That Actually Fits
Today, I work as an empowerment coach and host the On the Spectrum Empowerment Stories podcast—exactly the kind of relationship-based, healing-focused work Dr. Grey said autism made impossible.
His limiting beliefs about what autistic people can do were wrong. They reflected his biases, not reality.
For the complete, unfiltered story of my therapeutic journey, my book provides all the details.
Harmful Pattern #6: Telling You to Care What Everyone Thinks
The Detective Work
Dr. Grey started one session: "I wonder if perhaps there is a sign you are wearing that is pushing people away."
His solution: "This is where we need to do some detective work and get some feedback from others that could help us."
Later, when I shared feedback: "Well, let's listen to what these people are saying. You should care about what people say about you because this is what carried you throughout your whole life."
The Problem With This Approach
It reinforces external validation: Your worth becomes dependent on others' opinions rather than internal self-knowledge.
It ignores toxic sources: Feedback from people who called me "weird" and avoided me wasn't constructive—it was cruel.
It creates hypervigilance: Constantly monitoring others' reactions keeps you anxious and self-conscious.
It prevents authenticity: You can't be yourself while obsessing over everyone's judgments.
The Contradiction
Dr. Grey simultaneously wanted me to:
Care deeply about what everyone thinks
Develop confidence and self-worth
Be authentic while constantly performing for approval
These goals are incompatible.
What I Eventually Learned
The opinion of myself should count first. Not guys who rejected me. Not classmates who called me weird. Not even my therapist.
Building genuine self-worth requires:
Valuing your own assessment over others' judgments
Distinguishing between constructive feedback and cruel criticism
Developing internal standards rather than chasing external approval
Being selective about whose opinions you allow to matter
Ready to learn the complete story of navigating harmful therapy while struggling through law school? My book details every session, every harmful message, and what I eventually learned about genuine self-worth.
What Healthy Autism-Informed Therapy Actually Looks Like
The Positive Moments Were Real
Despite the harmful patterns, Dr. Grey did provide some valuable support:
CBT techniques: Teaching me to challenge all-or-nothing thinking and reframe negative thoughts like "Just because I never had a boyfriend doesn't mean I am nothing."
Validation of challenges: Acknowledging I had additional challenges other people didn't face because of autism and comorbid mood disorder.
Standing up for me: When family members suggested I was "cured" of autism or should stop therapy, he supported my continued treatment.
Advocacy against family misconceptions: Explaining that graduate school doesn't cure autism and therapy was keeping me afloat.
What Made Me Blind to the Problems
"This was where I blinded myself into thinking everything was okay with these therapy sessions: the fact that somebody understood autism."
When you've spent years with therapists who don't understand autism, finding someone who does feels like salvation. This can make you overlook significant problems with how they're applying that knowledge.
What Truly Helpful Autism Therapy Includes
Understanding autism without pathologizing it: Recognizing differences without framing them as deficits requiring compensation.
Building genuine self-worth: Internal validation that doesn't depend on appearance, dating success, or others' approval.
Consistent, non-contradictory messaging: Clear principles you can rely on to guide decisions.
Supporting authentic career paths: Helping you discover and pursue what genuinely calls to you, not limiting your options based on assumptions about autism.
Non-judgmental stance toward mental health: Creating safety rather than stigma around psychiatric diagnoses.
Balanced feedback processing: Teaching discernment about which opinions to consider versus which to dismiss.

How to Protect Yourself From Harmful Therapy
How to Protect Yourself From Harmful Therapy
Recognize the Warning Signs
Your therapy may be harmful if your therapist:
Makes you feel worse about yourself after sessions
Focuses obsessively on changing your appearance
Gives contradictory advice that keeps you confused
Reinforces that you must be "perfect" to compensate for autism
Stigmatizes mental health diagnoses
Limits your career aspirations based on assumptions about autism
Tells you to care what everyone thinks while claiming to build confidence
Trust Your Inner Voice
The moment I told Dr. Grey "I don't care what guys see me as. It's the opinion of myself that should count first" was pivotal.
Even in harmful therapeutic relationships, your inner wisdom knows truth. Listen to it.
You're Allowed to Push Back
Therapy isn't a one-way street where the expert dictates and you comply. You're allowed to:
Disagree with your therapist's assessments
Question advice that doesn't feel right
Express when something they said hurt you
Stop following guidance that makes you feel worse
Consider Whether the Relationship Is Worth Continuing
Ask yourself:
Is the helpful content worth the harmful messaging?
Am I staying because they understand autism, even though they're hurting me?
Would I tolerate this treatment from a friend or partner?
Is there someone else who could provide autism expertise without the harm?
Seek Second Opinions
If you're unsure whether your therapy is helpful or harmful:
Consult with another autism-informed therapist
Share specific examples with trusted people who know good therapy
Listen to your own emotional responses after sessions
Track whether you're getting better or worse over time
Listen to the On the Spectrum Empowerment Stories podcast for more insights on navigating therapeutic relationships, building genuine self-worth, and recognizing when support systems are helping versus harming.
Moving Forward From Harmful Therapy
The therapeutic relationship with Dr. Grey was complicated—moments of genuine support mixed with deeply harmful messaging that reinforced shame, perfectionism, and external validation.
The most important lesson: Specialization in autism doesn't guarantee good therapy.
What matters is:
How they apply their knowledge
Whether they build you up or tear you down
If they reinforce internal worth or external validation
Whether you feel better or worse after working with them
Today, I use my experience navigating harmful therapeutic relationships to help others recognize red flags earlier than I did. The years I spent absorbing harmful messages about needing to be perfect, thin, and acceptable took additional years to unlearn.
You don't have to repeat my mistakes. You can recognize harmful patterns early and find practitioners who truly support your authentic development.
For the complete, unfiltered story of my therapeutic journey through law school—including every harmful session, what kept me stuck, and how I eventually found genuine self-worth—my book provides all the details these takeaways only begin to address.

5 Signs You've Found the Right Therapist (And 3 Red Flags You're With the Wrong One)
Finding the right therapist can feel like searching for a needle in a haystack—especially when you're autistic, dealing with trauma, or struggling with issues that most practitioners don't fully understand. You show up vulnerable and desperate for help, only to leave sessions feeling dismissed, misunderstood, or worse than when you arrived.
Not all therapy is good therapy. Not all therapists are equipped to handle the specific challenges autistic people face. And sometimes, what sounds like helpful advice in the moment is actually reinforcing the exact patterns that are keeping you stuck.
After self-harm brought me to a breaking point in law school, my parents insisted I find therapeutic help. What followed was a journey through different practitioners—some who offered genuine insight, others who said things that were ultimately harmful, and eventually finding someone who understood both autism and the deeper work I needed.
This is about recognizing when you're getting real help versus when you're wasting time and money on therapy that isn't serving you.
Table of Contents
Good Sign #1: They Tell You Hard Truths You Need to Hear
Good Sign #2: They Help You Understand Patterns, Not Just Feelings
Good Sign #3: They Teach You Practical Self-Protection Skills
Good Sign #4: They Have Specific Expertise in Your Challenges
Good Sign #5: They See Your Bigger Picture, Not Just Your Symptoms
Red Flag #1: They Make Dismissive Statements About Your Struggles
Red Flag #2: They Tell You What You're "Meant" or "Not Meant" to Have
Red Flag #3: They Don't Specialize in What You Actually Need
How to Find the Right Therapeutic Support
Key Takeaways for Choosing Your Therapist
Moving Forward
Good Sign #1: They Tell You Hard Truths You Need to Hear
The Assignment You're Avoiding
After revealing my self-harm to my parents during their visit, they insisted I see a local therapist near law school. This therapist was willing to say something nobody else had directly addressed:
"We all have an assignment we have to do before our time is up on Earth. If you are feeling unfulfilled in a career path you are on, and it is more than just one bad day, then perhaps this is not your assignment."
Why This Matters
A good therapist doesn't just validate your feelings—they help you see uncomfortable truths you're avoiding.
In my case:
I was deeply unhappy in law school
The unhappiness wasn't temporary or situational
I was living a "brainwashed lie" of who I thought I needed to be
Law wasn't my assignment, but I was too scared to admit it
The Difference Between Hard Truth and Harsh Criticism
Hard truth:
Comes from a place of wanting you to live authentically
Helps you see patterns you've been denying
Gives you permission to make changes you're afraid to make
Focuses on your wellbeing, not others' expectations
Harsh criticism:
Focuses on what's wrong with you
Reinforces shame and inadequacy
Doesn't offer pathways forward
Makes you feel worse without clarity on what to change
A therapist who can deliver hard truths with compassion is helping you break through denial into authentic living.
When You're Too Scared to Hear It
At the time, I was too scared to act on this truth. The fear of disappointing parents, of admitting I'd chosen wrong, of having to start over—all of it kept me frozen.
But the therapist planted a seed. She named the reality I couldn't yet speak: You're in the wrong place, living the wrong life, and your suffering is telling you that.
Eventually, that truth became impossible to ignore.
Good Sign #2: They Help You Understand Patterns, Not Just Feelings
Beyond Surface Emotions
Good therapy doesn't just help you feel better temporarily. It helps you understand why things keep happening the way they do.
This therapist taught me about human behavior in ways that gave me a framework for understanding my experiences:
"People know whom to target and go after. It's like how sharks are able to detect their prey. People go after those whom they feel they can go after."
Why Pattern Recognition Matters
Understanding patterns helps you:
Recognize when you're being targeted rather than believing something is wrong with you.
Identify what makes you vulnerable to exploitation or mistreatment.
Make different choices based on understanding dynamics, not just reacting emotionally.
See your role in patterns without drowning in shame about it.
The Vulnerability You Carry
The therapist identified something crucial: "There is a vulnerability about you that you carry around."
This wasn't an insult. It was important information.
For autistic people, this vulnerability often comes from:
Social naivety that others can detect and exploit
Desperation for connection that makes you overlook red flags
Difficulty reading intentions, leaving you open to manipulation
Past trauma that hasn't been processed, creating visible wounds
Understanding this vulnerability is the first step toward protecting yourself from people who will take advantage of it.
Good Sign #3: They Teach You Practical Self-Protection Skills
More Than Just Awareness
Awareness without skills doesn't create change. A good therapist gives you specific strategies you can implement immediately.
This therapist taught me practical self-protection:
About keeping your head held up high: Physical posture matters. The way you carry yourself signals to others whether you're an easy target.
About standing up for yourself: Not just conceptually, but with specific language and boundaries.
About shutting down inappropriate topics: "If people talk about dating issues and are harping you for not being like them, you need to learn to start saying 'that is not up for discussion.'"
Why This Phrase Matters
"That is not up for discussion" is a complete sentence. It requires no explanation, no justification, no defense.
For autistic people who struggle with:
Over-explaining ourselves
Feeling obligated to answer every question
Not knowing how to set boundaries politely
Fearing we'll seem rude if we don't engage
This phrase is revolutionary. It's a boundary that protects you without requiring social finesse to execute.
Teaching About Red Flags
The therapist also helped me understand red flags in men's behavior with blunt honesty:
"A man who flirts with everyone is not special."
She explained that someone who behaves flirtatiously with everyone isn't showing you genuine interest—he's just operating from his natural pattern. The behavior means nothing about you specifically.
This helped me understand that Demetrious's flirtatiousness wasn't special attention. It was his standard operating procedure with everyone.
These kinds of practical skills and frameworks, explained in greater detail throughout my book, are what actually create change in your life, not just insight into why you feel bad.
Good Sign #4: They Have Specific Expertise in Your Challenges
When General Practice Isn't Enough
After attending an autism conference in Chicago, my parents heard keynote speaker Dr. Grey present on autism spectrum behaviors and social blindness. They were impressed by his specific knowledge about:
Repetitious patterns of behavior in autistic people
Social blindness and how it manifests
Autism-specific challenges in social situations
This led them to get his contact information, and I soon found myself in his office.
Why Specialization Matters
General therapists, however well-meaning, often:
Lack understanding of how autism affects everything from social interaction to emotional processing to sensory experiences.
Apply neurotypical frameworks that don't account for different neurological wiring.
Miss crucial context about why certain things are harder for autistic people.
Give advice that works for neurotypical people but fails for autistic clients.
What Autism-Specific Expertise Provides
A therapist with autism expertise:
Understands repetitious thought patterns as neurological, not just behavioral
Recognizes social blindness as a genuine processing difference
Doesn't pathologize autistic traits or try to make you "normal"
Offers strategies designed for how autistic brains actually work
Can distinguish between autistic traits and mental health conditions
When my parents saw Dr. Grey present with clear, specific knowledge about autism, they recognized this was expertise I needed access to. Watch out for these 7 Red Flags of Unethical Mental Health Practice when seeking care
Good Sign #5: They See Your Bigger Picture, Not Just Your Symptoms
Beyond the Presenting Problem
I came to therapy because of self-harm. But good therapists understand that surface behaviors always point to deeper issues.
The self-harm wasn't the problem. It was a symptom of:
Being in a career path that wasn't mine
Years of unprocessed rejection and trauma
Lack of genuine self-worth
Trying to be someone I wasn't to meet others' expectations
Accumulated pain with no healthy outlet
What "Seeing the Bigger Picture" Means
A therapist who sees your bigger picture:
Connects current struggles to past experiences rather than treating each problem in isolation.
Understands how different issues intersect—autism, trauma, depression, social isolation, career dissatisfaction.
Addresses root causes instead of just managing symptoms.
Helps you see patterns across your life that explain why you're stuck.
Works toward authentic living rather than just reducing distress.
The Question of Your Assignment
When the therapist said "perhaps this is not your assignment," she was seeing the bigger picture:
My unhappiness wasn't just about one bad semester
Law school was the wrong path for my authentic self
I was living according to others' expectations, not my own values
The pain would continue until I aligned with my true assignment
This is deeper work than "how do I feel better in law school." This is "why are you in law school in the first place?"
Red Flag #1: They Make Dismissive Statements About Your Struggles
When Good Advice Turns Harmful
The same therapist who offered valuable insights also said things that were ultimately dismissive:
"You aren't meant to have friends right now." "You aren't meant to have a boyfriend." "You could've had a boyfriend years ago."
Why These Statements Are Harmful
They dismiss the real struggle of being autistic in a neurotypical social world.
They frame isolation as destiny rather than addressing the barriers preventing connection.
They suggest you should accept loneliness rather than working to build genuine relationships.
They lack empathy for how painful social isolation actually is.
They offer no pathway forward—just acceptance of a painful reality.
The Impact of Dismissive Statements
Hearing "you aren't meant to have friends right now" when you're desperately lonely:
Reinforces that something is fundamentally wrong with you
Suggests your desire for connection is the problem
Provides no skills for building the friendships you need
Makes isolation feel permanent and unchangeable
These statements felt like the therapist was giving up on the possibility of my social life improving, rather than helping me understand what needed to change to make improvement possible.
What Should Have Been Said Instead
A more helpful approach:
"Building friendships is challenging for autistic people, and it requires specific skills and strategies. Let's work on those."
"The relationships you've had haven't been healthy. Let's focus on what genuine friendship looks like and how to recognize it."
"Your current social strategies aren't working. Here's what we can try differently."
Red Flag #2: They Tell You What You're "Meant" or "Not Meant" to Have
The Problem With Destiny Language
Saying someone is "meant" or "not meant" to have something removed agency and suggests their circumstances are fixed and unchangeable.
This language is particularly harmful for autistic people who:
Already feel fundamentally different and broken
Struggle with social connections that seem effortless for others
Wonder if they're capable of the relationships they see others have
Need to believe change is possible to keep trying
What This Language Communicates
"You aren't meant to have friends right now" communicates:
Your loneliness is somehow cosmically ordained
There's nothing you can do about it
Wanting friends is futile or misguided
You should accept isolation as your fate
This is the opposite of empowering therapeutic language.
The Alternative
Empowering therapeutic language:
"Your current approach to friendships hasn't worked. Let's figure out why and try something different."
"Building authentic connections takes time and specific skills. Here's what we'll work on."
"You haven't yet built the friendships you want, but that doesn't mean you can't. Here's how we'll get there."
This language maintains hope while being realistic about the work required.
Red Flag #3: They Don't Specialize in What You Actually Need
The Generalist Problem
Many therapists are trained in general mental health support but lack specific expertise in:
Autism spectrum disorders
Trauma-informed approaches
Self-harm and crisis intervention
Social skills development for autistic adults
Career and identity issues
When your challenges span multiple specialized areas, a generalist may provide surface-level support without addressing the depth of what you're dealing with.
Why My Parents Sought Dr. Grey
After hearing Dr. Grey speak specifically about:
Autism spectrum behaviors
Social blindness
Repetitious patterns in autistic people
My parents recognized this was specialized knowledge I needed access to. His expertise wasn't just general therapy—it was autism-specific understanding.
The complete story of my therapeutic journey, including what eventually worked with Dr. Grey and other practitioners, is detailed in my book. Understanding what to look for in therapy can save you years of ineffective treatment.
How to Find the Right Therapeutic Support
Step 1: Identify What You Actually Need
Before searching for a therapist, clarify:
Do you need autism-specific expertise?
Is trauma a primary concern?
Are you dealing with specific issues like self-harm or crisis?
Do you need help with social skills, relationships, or life direction?
What hasn't worked in past therapy?
Be specific. "I need someone who understands autism" is better than "I need therapy."
Step 2: Research Specializations
Look for therapists who specifically list:
Autism spectrum disorders (especially adult autism)
Trauma-informed care
CBT, DBT, or other evidence-based approaches
Experience with your specific demographic
Don't settle for "general mental health" if you need specialized support.
Step 3: Ask Direct Questions in Initial Consultations
In your first session or consultation call, ask:
"What experience do you have working with autistic adults?"
"How do you approach social skills development?"
"What's your understanding of how autism affects relationships?"
"Have you worked with clients dealing with [your specific issue]?"
Their answers will tell you if they have real expertise or are winging it.
Step 4: Trust Your Gut About Fit
Even a qualified therapist might not be the right fit for you. Pay attention to:
Do you feel understood or constantly misunderstood?
Are they teaching you new skills or just validating feelings?
Do you leave sessions with clarity or more confusion?
Are they dismissive or empowering?
Do they see your potential or just your deficits?
Step 5: Don't Stay With the Wrong Therapist Out of Obligation
If therapy isn't helping after several sessions, it's okay to:
Tell them it's not the right fit
Ask for a referral to someone more specialized
Simply stop scheduling and find someone new
You don't owe anyone your time and money when they're not serving you well.
Step 6: Look for These Green Flags
The right therapist:
Tells you hard truths with compassion
Teaches practical skills, not just provides support
Has specific expertise in your needs
Sees your bigger picture, not just symptoms
Empowers rather than dismisses
Makes you feel hopeful about change, not hopeless about your circumstances
Get your copy of Dropped in a Maze: My Life On The Spectrum today.
Key Takeaways for Choosing Your Therapist
Good Therapy Challenges You to Grow
The therapist who told me "perhaps this is not your assignment" was challenging me to admit an uncomfortable truth. That's good therapy—not comfortable, but necessary.
Dismissive Language Reveals Underlying Attitudes
When a therapist says "you aren't meant to have friends right now," they're revealing they don't believe in your capacity for change in that area. That's a problem.
Specialization Matters for Complex Needs
Autism plus trauma plus social struggles plus career crisis requires more than general counseling. Seek specialists who understand your specific constellation of challenges.
You Can Switch Therapists
Just because you started with someone doesn't mean you're obligated to stay. If it's not working, find someone better suited to your needs.
Trust Takes Time, But Dismissiveness Happens Fast
Give a new therapist a few sessions to build trust and understand your situation. But if they're dismissive or harmful from the start, that's unlikely to improve.
The Right Therapist Sees Your Potential
Not just your problems, not just your diagnosis, not just your current struggles—but who you could become with the right support.
Moving Forward
Finding the right therapist transformed my trajectory. The wrong therapists provided surface support, made dismissive comments, or lacked the specific expertise I needed. But the practitioners who understood autism, could deliver hard truths with compassion, and taught practical skills made real change possible.
If you're currently in therapy that isn't helping, know that it's not that therapy doesn't work—it's that you haven't yet found the right therapeutic approach or practitioner for your specific needs.
Ready to learn the complete story of navigating therapy as an autistic person in crisis, my book provides everything you need to make informed choices about your own therapeutic journey.
Get your copy of Dropped in a Maze: My Life On The Spectrum today.

Why Autistic People Struggle With Romantic Relationships
Everyone around you seems to be dating. Getting into relationships. Moving on from breakups and finding someone new within weeks. And there you are, wondering why something that appears so effortless for others feels completely out of reach for you.
For autistic people, romantic relationships aren't just emotionally complicated—they involve a layer of confusion, missed signals, and unprocessed pain that neurotypical people rarely have to navigate. The social rules of dating are already complex. For someone who struggles to read between the lines, misses subtle cues, and has spent years being rejected and mistreated, romantic connection can feel like climbing Mount Everest while everyone else takes the elevator.
This blog post addresses what nobody talks about when it comes to autism and romantic relationships—the real reasons why dating is harder, what happens when that pain goes unaddressed, and what you genuinely need to hear if you're struggling right now.
If you or someone you know is struggling with self-harm or mental health crisis, please contact the 988 Suicide and Crisis Lifeline by calling or texting 988. You are not alone.
Table of Contents
Reason #1: You're Reading Flirtatious Signals as Romantic Interest
Reason #2: Past Rejection Follows You Into New Situations
Reason #3: Dating Milestones Feel Like a Report Card
Reason #4: You're Looking for Answers in the Wrong Places
Reason #5: The Pain of Unmet Needs Reaches a Breaking Point
Reason #6: Nobody Around You Truly Understands
What You Actually Need (Not What People Tell You)
Key Takeaways for Autistic People Navigating Romance
Reason #1: You're Reading Flirtatious Signals as Romantic Interest
The Mixed Signal Problem
One of the most painful experiences in romantic relationships is when someone acts flirtatious—playful physical contact, consistent eye contact, warm smiles—and then completely withdraws when you show genuine interest.
For autistic people, this is particularly devastating because we tend to take behavior at face value. If someone acts as though they like us, we believe they like us. We don't automatically factor in that some people are naturally flirtatious with everyone, or that someone can enjoy the attention of a person they have no actual romantic interest in.
Why Autistic People Miss These Cues
We process social information differently. The subtle distinction between "being friendly" and "being interested" involves reading a complex combination of context, consistency, body language, and social patterns that don't always compute the same way for autistic people.
We have less experience to draw from. Neurotypical people develop romantic intuition through years of casual dating experiences that teach them how to read signals. Without that foundation, every interaction feels like the first time.
We take behavior literally. When someone pats you on the back, shoves your chair playfully, and smiles every time they see you, the logical conclusion is that they're interested. Detecting the subtle difference between flirting for fun and genuine romantic interest requires reading invisible social rules.
We don't factor in inconsistency as rejection. When someone waits three days to respond to a dinner invitation and then declines without suggesting an alternative time, a neurotypical person recognizes this as a clear "no." An autistic person may miss this indirect signal entirely.
The Cruel Reality
What hurts most isn't just the rejection itself. It's not understanding why someone who behaved warmly and flirtatiously could turn around and express no romantic interest. This disconnect—between observed behavior and actual intention—is deeply confusing for autistic people.
The confusion keeps you stuck, trying to decode what happened instead of moving forward.
In my book, I detail the complete story of navigating this exact confusion in law school and the specific strategies that could have helped me recognize these signals earlier. Understanding this pattern can save you enormous pain.
Reason #2: Past Rejection Follows You Into New Situations
The Backpack of Past Pain
Every rejection you've experienced doesn't just disappear. It gets packed into a mental backpack you carry into every new situation.
Years of being rejected, bullied, and told you're not good enough create automatic fear responses:
Fear of asking for someone's phone number in case they laugh at you
Backing out of social situations at the last minute to avoid potential humiliation
Assuming new rejections confirm old messages about your worth
Being unable to distinguish between a new person and past people who hurt you
The Freeze Response
When you want to ask someone for their number but the memory of past humiliation kicks in, your body responds as if the past rejection is happening right now. You freeze. You avoid. You miss the opportunity entirely.
This isn't weakness or lack of confidence. It's a trauma response to repeated painful experiences. Your nervous system learned that social risk means pain, and it's trying to protect you.
Why This Is Different for Autistic People
Autistic people often have:
Longer processing times for social trauma. Neurotypical people may recover from romantic rejection more quickly. For autistic people, who tend to perseverate on difficult experiences, rejection can stay active in the mind for much longer.
Deeper sensitivity to rejection. Many autistic people experience rejection sensitive dysphoria—an intense emotional response to perceived rejection that goes beyond typical hurt feelings.
Less resilience from positive experiences. Without a history of positive romantic experiences to balance the negative ones, each rejection carries disproportionate weight.
Difficulty separating past from present. Clinging to past memories of how people treated you prevents you from recognizing that you're not the same person you were, and that new people aren't the same as the ones who hurt you.
Reason #3: Dating Milestones Feel Like a Report Card
The Comparison Trap
When everyone around you is dating, getting into relationships, and progressing through romantic milestones, not participating in any of these experiences can feel like failing a test everyone else passed.
At law school, when classmates found out I'd never had a boyfriend or been on a date, they were flabbergasted. Some said there was a big part of social life missing in not dating. Comments about singlehood—even well-meaning ones—stacked on top of each other until singlehood felt like a character flaw.
Why Milestones Hurt More for Autistic People
We're already behind on other social milestones: If you've spent your whole life feeling behind your peers socially, romantic milestones become yet another measure of how far you've fallen short.
Society treats romantic experience as a marker of worth: The messaging is everywhere: having a partner means you're likable, attractive, socially successful. Not having one means something is wrong with you.
Autistic people often have delayed development in these areas: This isn't a personal failing—it's a natural result of processing the world differently. But without that context, the gap between your experience and your peers' experience feels deeply personal.
You compare your insides to others' outsides: You see friends walking arm in arm with partners and assume their romantic lives are easy and fulfilling. You don't see the complexity behind what looks effortless from the outside.
The Arranged Match Expectation
For some autistic people—particularly those from cultures with arranged marriage traditions—there's an additional pressure that romantic connection will simply be "handled" by family. But arranged setups don't guarantee anything. People still have to genuinely like each other. And when you've spent years struggling to connect with people, the additional pressure of arranged introductions only amplifies the anxiety.
What everyone needs, above all, is to be genuinely loved for who they truly are. Not strategic matches, not arrangements, not someone tolerating them out of obligation. Genuine love.
Reason #4: You're Looking for Answers in the Wrong Places
The Decoding Obsession
After a painful rejection, it's natural to want to understand what happened. But when the search for answers becomes obsessive, it can take over your life.
Constantly asking others "What does it mean when a guy leads a woman on?" or trying to decode every text and interaction keeps you stuck in the past instead of moving forward. Every person you ask has a different opinion, which creates more confusion rather than clarity.
Why Autistic People Get Stuck Here
We're natural pattern-seekers. Autistic brains are wired to find logic and patterns. When someone's behavior doesn't make logical sense, we keep analyzing until we find an explanation.
We want a definitive answer. Uncertainty is deeply uncomfortable for many autistic people. "Maybe he just wasn't that interested" doesn't satisfy because it leaves too many unknowns.
We look externally for validation we need internally. The real question isn't "What's wrong with me that he rejected me?" The real work is building enough internal self-worth that one person's rejection doesn't define your value.
The Karaoke Coping Mechanism
During this painful period, I was drinking to excess on weekends, doing impersonations of professors at parties, and performing raunchy raps at birthday dinners—all channeling pain into performances for others' entertainment.
This was the same pattern from middle school: using performance as a way to connect, to get people to like you, to find belonging through entertainment.
It wasn't healthy connection. It was pain wearing a costume.
What You're Actually Looking For
The search for answers about why someone rejected you is really a search for:
Confirmation that you're worthy of love
An explanation that doesn't make you the problem
Permission to stop blaming yourself
Evidence that you're likable, valuable, and enough
These things cannot come from the person who rejected you. They have to come from within—which requires deep therapeutic work that goes far beyond surface-level coping.
Reason #5: Nobody Around You Truly Understands
The Isolation of Being Misunderstood
Even when surrounded by people, the autistic experience of romantic struggle can feel profoundly isolating because nobody around you truly gets it.
Friends say:
"Just ask him out"
"You need to give guys a chance"
"Brush it off and move on"
"Everybody goes through this"
These responses, however well-meaning, miss the entire context of what you're actually dealing with:
Years of accumulated rejection
Difficulty reading social and romantic signals
Unprocessed trauma from bullying and social failure
A nervous system that responds to social risk with intense fear
A brain that processes relationships differently than neurotypical people
The Disclosure Dilemma
I didn't disclose my autism diagnosis to people at law school for a long time, out of fear of hearing: "If you have autism, you shouldn't be in the legal profession."
This fear kept me from explaining behaviors that looked like flakiness or indecision to others—like backing out of plans due to sensory overload—but were actually neurological responses to overwhelm.
Not being able to explain yourself creates a painful double bind:
Don't disclose: people misread your behavior and get frustrated
Disclose: risk judgment, discrimination, and reduced expectations
When Disclosure Happens
When I finally told Khloe and Natalia about my autism diagnosis, Natalia's response was: "It makes sense why you didn't get Demetrious's number yet."
That response reduced all the complexity of living with autism to one social behavior. It missed the much bigger picture of what autistic people navigate in every interaction, every day.
Finding people who see the full picture—not just the narrow slice that affects them—is rare. But those people exist, and they're worth finding. Also, if you are finding it hard to make friends, this blogpost will help you navigate friendships as well.
What You Actually Need (Not What People Tell You)
What People Tell You
"Just put yourself out there"
"Confidence is attractive, just be confident"
"You're too picky"
"Stop overthinking it"
"Everyone gets rejected, just move on"
What You Actually Need
Trauma-informed therapeutic support Not just someone to vent to, but a therapist trained in both autism and trauma who can help you process the years of rejection and build genuine self-worth.
Social skills coaching specific to dating General social skills training is different from navigating the specific complexity of romantic interest, mixed signals, and rejection. Targeted coaching for this specific area matters.
Community with other autistic people Connecting with others who share your experience validates that your struggles are real and not personal failings.
Time to develop at your own pace Romantic development for autistic people happens on a different timeline. That's not a deficiency—it's a different path.
Self-compassion as a practice Not just hearing that you're worthy, but doing the internal work to genuinely believe it. This is the foundation everything else is built on.
Realistic expectations about what relationships require Genuine love—being loved for who you truly are—is what matters. Not arrangements, not someone tolerating you, not someone who makes you feel like you have to fight for basic acceptance.
Get your copy of Dropped in a Maze: My Life On The Spectrum today.
Key Takeaways for Autistic People Navigating Romance
Mixed Signals Are a Real Problem, Not Your Imagination
When someone's behavior doesn't match their level of romantic interest, that's genuinely confusing for anyone. For autistic people, it's especially difficult. You're not broken for missing these signals. You're working with a different social processing system in a world that doesn't explain its rules.
Past Rejection Is Not Your Future
The fear response that keeps you from asking for a phone number or accepting a dinner invitation is based on past pain, not present reality. You have grown. You are not the same person who was bullied and rejected in middle school. New people are not the same people who hurt you.
Milestones Are Not Measurements of Worth
Never having dated by your twenties does not mean something is wrong with you. It means your development followed a different timeline. The meaning you assign to it matters more than the fact itself.
Surface-Level Support Is Not Enough
If you've been in therapy and still feel stuck, it may not be that therapy doesn't work for you—it may be that you haven't yet found the right therapeutic approach. Keep looking for a practitioner who understands both autism and trauma at a deep level.
Your Pain Is Valid and Deserves Real Help
Being told to "brush it off" when you're carrying decades of accumulated pain is not support. Your pain is real. It has real roots. It deserves real, substantive help—not dismissal.
You Deserve to Be Loved for Who You Are
Not tolerated. Not accommodated. Not chosen for strategic reasons.
Loved—genuinely and authentically—for exactly who you are.
That kind of love exists. But it starts with doing the internal work to know who you are and believe you're worthy of it.
Final Thoughts
Romantic relationships are hard for everyone. But for autistic people carrying years of rejection, trauma, and social confusion, they can feel impossible.
The struggles aren't personal failings. They're the natural result of navigating a neurotypical world's unspoken rules without the social blueprint that neurotypical people receive through years of casual romantic experience.
Ready to read the complete, unfiltered story of struggling with romantic relationships, rejection, and mental health as an autistic person in law school? My book doesn't sugarcoat the pain or skip the hard parts. It tells the full truth—and offers the wisdom that came from surviving it.
Get your copy of Dropped in a Maze: My Life On The Spectrum today.

7 Signs You've Become the Toxic Person (And How Depression Makes It Worse)
Nobody wants to admit they've become toxic. We're quick to identify toxic people in our lives, but recognizing when we're the problem? That's devastatingly hard.
Depression doesn't just make you sad—it can turn you into someone who drains others, dumps emotions on people who aren't equipped to handle them, and pushes away the few genuine connections you have. Add unprocessed trauma from years of rejection and bullying, and you become a walking red flag to anyone who might have been your friend.
This is the uncomfortable truth I had to face after my 21st birthday disaster. The depression that followed didn't just make me miserable—it made me toxic to be around. I became the person others avoided, the one who brought negative energy into every interaction, the friend who took without giving back.
For autistic people struggling with depression after years of social failure, this pattern is particularly dangerous. We already struggle with social skills. When depression turns us toxic, we destroy the few chances we have at genuine connection.
This is about recognizing when you've crossed the line from struggling to toxic—and what you need to do differently to heal.
Table of Contents
Sign #1: You're Emotionally Dumping on Acquaintances
Sign #2: You Can't Stop Talking About Your Pain
Sign #3: Your Envy of Others' Friendships Poisons Interactions
Sign #4: You Obsess Over One Topic Despite People's Discomfort
Sign #5: You Stand People Up or Cancel Because of Your Mood
Sign #6: You Can't Pull Yourself Out of Depression Alone
Sign #7: You're Disconnected From Yourself and Your Needs
How to Stop Being Toxic and Start Healing
Key Takeaways for Breaking the Cycle
Sign #1: You're Emotionally Dumping on Acquaintances
What Emotional Dumping Looks Like
After my birthday disaster, something strange started happening. Sapna, one of the people who'd bailed on my celebration, began encouraging me to vent to her about what was going on.
I took her up on it. I would share my frustrations, cry about how things turned out, and unload all my pain onto her.
This wasn't healthy communication. This was emotional dumping on someone who wasn't actually my close friend.
The Difference Between Sharing and Dumping
Healthy sharing:
Reciprocal conversations where both people contribute
Appropriate to the relationship depth
Includes positive interactions, not just problems
Respects the other person's emotional capacity
Happens with people who've explicitly offered support
Emotional dumping:
One-sided unloading of problems and pain
Too intense for the relationship level
Happens repeatedly without reciprocation
Ignores whether the other person can handle it
Treats acquaintances like therapists
Why This Is Toxic
Emotional dumping:
Burdens people who didn't sign up for it. Acquaintances aren't equipped to handle your deepest trauma and pain.
Creates imbalanced relationships. You're taking emotional support without giving anything back.
Pushes people away. Even people who initially felt sympathetic will start avoiding you.
Prevents real friendships from forming. People see you as needy and draining before getting to know you.
What I Should Have Done Instead
Looking back, I recognize that my pain was my responsibility to bear, not Sapna's to carry. I owed her an apology for the emotional dumping.
What I needed:
A therapist trained to handle that level of pain
Processing past trauma, not just surface emotions
Skills for managing depression, not just people to vent to
Healthy boundaries about what to share and with whom
Dropped in a Maze: My Life On The Spectrum
Sign #2: You Can't Stop Talking About Your Pain
The Depression That Clung Like an Octopus
The Fall 2003 semester was numbing and depressing. Every day felt like struggling to stay above water. The feelings from my birthday—anger, hurt, betrayal, self-loathing—clung to me like an octopus clinging to a face.
I couldn't shake it off. Worse, I couldn't stop talking about it.
When Pain Becomes Your Identity
Depression can make your pain become the only thing you can talk about:
Every conversation circles back to your struggles. No matter what topic starts the discussion, you redirect it to your pain.
You can't engage with others' lives. When people share their experiences, you immediately relate it back to your own suffering.
Happy moments feel impossible. Even when good things happen, you can't fully experience them because depression clouds everything.
You become a black hole of negativity. People start to dread interactions with you because they know it'll just be more pain.
The Triggering Environment
It didn't help that birthday conversations were happening constantly around me. People were:
Going on trips with friends for their birthdays
Having dinner celebrations
Throwing parties they were excited about
None of which included eating a fish sandwich alone at a fast-food place.
Every conversation about birthdays was a trigger that sent me spiraling back into the shame and embarrassment of my own experience.
Why This Pushes People Away
When you can't stop talking about your pain:
People feel helpless. They don't know how to help and feel bad that nothing they say makes a difference.
Interactions become exhausting. Every conversation requires emotional labor they're not getting paid for.
They start avoiding you. It's not personal—they're protecting their own mental health.
You miss opportunities to connect. Shared interests and positive experiences are what build friendships, not shared misery.
What's Actually Needed
My therapist, Dr. Theroux, kept validating my feelings: "Anybody who was in a similar situation to you would also feel devastated to feel that nobody was close enough to celebrate them."
But validation alone wasn't enough. She also kept telling me to "pull myself out of the depression."
I tried. I couldn't. I didn't have the skills.
What I actually needed was deeper therapeutic work on:
Processing childhood trauma that the birthday triggered
Learning to love myself, which I had no clue how to do
Developing skills to manage intense emotions
Healing the root causes, not just managing symptoms
In my book, I detail the complete struggle with depression during this semester and what eventually helped me move beyond just talking about pain to actually healing from it. Understanding this difference is crucial for anyone stuck in this pattern.
Sign #3: Your Envy of Others' Friendships Poisons Interactions
The Toxic Combination
When I vented to Sapna, I wasn't just expressing sadness. I was emotionally dumping while simultaneously being envious that she had friends despite sharing her own childhood difficulties.
Sapna emphasized how hard she worked to get friends. I kept thinking I was doing the same thing, and that aggravated me.
The anger was really about my own frustrations, but it poisoned our interactions.
How Envy Shows Up
Envy in friendships manifests as:
Resentment when others succeed socially. Instead of being happy for them, you feel bitter about your own situation.
Comparing constantly. "Why do they have friends and I don't? What's wrong with me?"
Inability to celebrate others. Their wins feel like your losses.
Passive-aggressive comments. Subtle digs that reveal your jealousy.
Taking their friendship for granted. You're so focused on what you lack that you don't appreciate what you have.
Why This Is Toxic
Envy:
Creates negative energy that people can feel even if you don't voice it.
Prevents genuine connection because you're focused on what you don't have rather than building what's in front of you.
Makes people feel bad about their own happiness around you.
Reveals that you're using them as a measuring stick for your own inadequacy rather than valuing them as individuals.
The Reality Check
The truth was Sapna and I were both unhealthy in our own ways. I had no business emotionally dumping on her, and my envy made the dynamic even more toxic.
Her having friends didn't take anything away from me. But depression and unprocessed trauma made it feel that way.
Sign #4: You Obsess Over One Topic Despite People's Discomfort
The Sorority Fixation
During Fall 2003, my interest in joining a sorority grew. I thought if I was part of one, I would finally learn how to be likable and have friends.
I saw sorority girls dressed impeccably with nice outfits, hair done, and makeup on. I wished I could look like them and be like them.
I talked about sorority life constantly with Savannah, who was actually in a sorority, until she finally snapped.
When She Called Me Out
"This is why I get so irritated every time I talk to you! You always talk about sorority life," Savannah exclaimed.
"Oh, I am so sorry! I didn't realize," I said, feeling horrible.
"Nobody really talks about sororities much anymore. I'm about to graduate. Nobody even brings up sorority stuff anymore."
Why This Happens
Autistic people often develop intense interests that we want to discuss constantly. When that interest is tied to social belonging we desperately want, it becomes even more consuming.
I didn't realize I was:
Bringing it up in every conversation
Ignoring Savannah's discomfort with the topic
Making her feel like I only valued her for sorority information
Being tone-deaf about what was appropriate to discuss
The Impact
Obsessing over one topic:
Makes people feel like you're not interested in them as individuals, only as resources.
Creates irritation and frustration that builds over time until they explode.
Signals poor social awareness that makes people wary of deeper friendship.
Prevents balanced conversations that could actually build connection.
How to Recognize the Pattern
Warning signs you're doing this:
People change the subject when you bring up your topic
Someone explicitly tells you to stop talking about it
You notice yourself steering every conversation back to one thing
People start avoiding certain topics around you because they know you'll hijack the conversation
Sign #5: You Stand People Up or Cancel Because of Your Mood
The Pattern With Sapna
Sapna and I made plans throughout the semester to hang out on weekends. Most often, I would be stood up.
This was bewildering because she encouraged vulnerable conversations but then wouldn't follow through on plans.
When Depression Controls Your Reliability
Being stood up is toxic behavior. But depression can also make you:
Cancel plans last minute because you can't handle leaving your room.
Not show up because your mood tanked and you couldn't face socializing.
Make commitments you can't keep because you feel better in the moment but crash later.
Flake repeatedly without explanation, leaving people confused and hurt.
Why This Destroys Relationships
Unreliability:
Shows people they can't count on you. Trust is built on consistency.
Wastes their time when they've arranged their schedule around you.
Creates resentment that builds with each cancellation.
Signals that your needs always trump theirs, which isn't sustainable in friendship.
The Missing Piece
I missed the social cue that this wasn't a genuine friendship. Sapna was more of an acquaintance, and I should have recognized that earlier.
But the pattern of unreliability—whether from her, from me, or both—prevented anything deeper from forming.
Sign #6: You Can't Pull Yourself Out of Depression Alone
The Therapist's Impossible Advice
Dr. Theroux kept telling me to "pull myself out of the depression."
I tried so hard. I couldn't do it. I didn't have the skills.
My emotions ate me up every day. I had major crying outbursts when alone. Sometimes tears would well up during class.
Why "Pull Yourself Out" Doesn't Work
Depression isn't a choice. You can't just decide to feel better any more than you can decide to cure a broken leg through positive thinking.
What doesn't work:
Telling yourself to snap out of it
Trying harder to be happy
Forcing yourself to socialize when you're empty inside
Pretending everything is fine
What's actually needed:
Deep therapeutic work on root causes, not just surface symptoms
Processing past trauma that the current situation triggered
Learning specific skills for emotional regulation and self-compassion
Sometimes medication to address chemical imbalances
Time and patience with the healing process
The Childhood Connection
What really needed to be worked on was processing the past and how it affected my present situation. I needed to learn how to heal and how to love myself. I hadn't the first clue how to do that.
The embarrassment and shame from my 21st birthday traced all the way back to childhood:
Years of rejection and bullying
Being made to sit alone at events
Constant social failure and isolation
Messages that I was unworthy and should be destroyed
You can't "pull yourself out" of depression rooted in decades of trauma without addressing the trauma itself.
What Changed Things
The intense depression lasted the entire Fall 2003 semester. The only times I felt somewhat "normal" were when I hung out with others at bars in The Village, where I felt like part of the group—even if it was just a facade.
Real change didn't come from trying harder. It came from:
Getting a new start in Spring 2004
Meeting people like Leslie who asked the right questions
Learning healthier connection patterns over time
Eventually doing deeper therapeutic work (though not until much later)
The complete story of struggling with this depression and what eventually helped me move beyond it is detailed in my book. If you're stuck in this pattern, understanding what actually works versus what well-meaning therapists tell you to do can save you years of suffering.
Sign #7: You're Disconnected From Yourself and Your Needs
The Missing Connection
During this time, I was focused entirely on:
Making friends
Being accepted
Learning to be likable
Looking like the sorority girls
Having what others had
What I wasn't focused on: myself. Who I actually was. What I actually wanted.
The Void at Graduation
I graduated college feeling a void because I knew I was about to enter a career I didn't have a sincere heart for.
Even though I would've still had social challenges, I believe the edges of loneliness and the overall college experience would've been better if I had listened to my own heart.
That would've meant:
Exploring psychology or journalism—courses I would've enjoyed
Taking classes aligned with my interests
Feeling connected to what I was studying
Becoming connected to the most important person: myself
Why Self-Disconnection Makes You Toxic
When you're disconnected from yourself:
You can't offer authentic connection because you don't know who you authentically are.
You seek validation externally instead of building internal self-worth.
You try to be what others want rather than discovering what you want.
You create relationships based on need rather than genuine compatibility.
You don't have boundaries because you don't know what you need or value.
The Real Work
The real connection missing was the one I had with myself. All the social skills training in the world won't fix that fundamental disconnection.
True healing requires:
Learning who you are beyond others' expectations
Discovering your own interests and passions
Building self-worth from internal sources
Honoring your needs, not just accommodating others
Making choices aligned with your authentic self
How to Stop Being Toxic and Start Healing
Step 1: Recognize You Can't Do This Alone
Stop trying to "pull yourself out of depression" through willpower. You need:
A therapist trained in trauma who can help you process the root causes
Support groups with people who understand what you're experiencing
Possibly medication if depression has a chemical component
Time and patience with the healing process
Depression rooted in trauma requires professional help, not just positive thinking.
Step 2: Stop Emotional Dumping on Acquaintances
Create clear boundaries about what you share and with whom:
Acquaintances: Surface-level updates, no deep trauma Developing friends: Some challenges, balanced with positive interactions Close friends: Deeper struggles, but still reciprocal and boundaried Therapists: The full weight of trauma and pain
Your pain is your responsibility to heal, not others' to carry.
Step 3: Learn to Sit With Envy Without Acting on It
Envy is a normal human emotion. The problem is when you:
Let it poison your interactions
Express it through passive-aggressive comments
Use it as fuel for resentment
Instead:
Acknowledge the envy to yourself
Recognize it's about your pain, not their success
Use it as information about what you want
Don't let it leak into the relationship
Step 4: Monitor How Often You Bring Up Your Obsessions
Pay attention to:
How often you steer conversations to your topic of interest
Whether people seem uncomfortable or change the subject
If you're asking about others' lives or just talking about yours
When someone explicitly tells you to stop
Make a conscious effort to:
Ask questions about the other person
Let them lead some conversations
Notice when you're dominating with one topic
Diversify what you talk about
Step 5: Be Reliable or Don't Make Plans
If depression makes you unreliable:
Option 1: Only commit to plans when you're reasonably sure you can follow through
Option 2: Be honest about your limitations: "I'd like to make plans, but I'm dealing with depression and might need to cancel. Is that okay with you?"
Option 3: Stick to low-commitment hangouts that don't require advance planning
Don't repeatedly stand people up or cancel last minute. It destroys trust.
Step 6: Process Trauma, Don't Just Manage Symptoms
Surface-level therapy that validates feelings without addressing root causes won't create lasting change.
You need to:
Process childhood experiences that created current patterns
Understand how past trauma affects present relationships
Heal the wounds, not just bandage the symptoms
Learn new patterns based on self-worth, not desperation
This takes time and the right therapeutic approach.
Step 7: Reconnect With Yourself
Ask yourself questions you've been avoiding:
What do I actually enjoy?
What interests me beyond social acceptance?
What would I study if I weren't trying to please others?
Who am I when I'm alone?
What do I value and need?
Build a relationship with yourself before expecting others to have relationships with you.
If you're autistic, Sonia's podcast offers essential guidance on finding ethical mental health support
Key Takeaways for Breaking the Cycle
Toxicity Often Comes From Unprocessed Pain
You're not a bad person for becoming toxic. You're a hurt person who hasn't healed, acting out of that pain in ways that push people away.
Recognizing this is the first step toward change.
Depression Makes Everything Harder
When depression tells you to "just try harder," remember:
Depression is a liar
You can't think your way out of clinical depression
Professional help isn't weakness—it's necessary
Healing takes time and appropriate treatment
Some Friendships Form Despite Your Struggles
During Spring 2004, healthier friendships started forming:
Leslie arrived as my new roommate and asked insightful questions about my autism diagnosis that showed she understood.
Carrie connected with me on deeper intellectual levels and shared her own healing journey, introducing me to books like The Four Agreements.
These friendships were testament to never giving up on making connections, even when depression made it feel impossible.
The Most Important Connection Is With Yourself
All the social skills in the world won't fix fundamental self-disconnection.
Learning to:
Know yourself
Honor your interests
Make choices aligned with your authentic self
Build internal self-worth
These are prerequisites for genuine, healthy connections with others.
Ready to learn the complete journey from toxic patterns to healthy friendships? Get a copy of dropped in a Maze today and learn how to break the cycle of toxicity rooted in unprocessed pain.
Moving Forward
The Fall 2003 semester was one of the darkest periods of my life. I became someone I'm not proud of—emotionally dumping on acquaintances, unable to stop talking about pain, envious of others' friendships, obsessing over sororities, and disconnected from my authentic self.
But recognizing these toxic patterns was the beginning of change. Spring 2004 brought new friendships with Leslie and Carrie that showed me what healthy connection could look like.
Eventually, I learned that:
Emotional dumping isn't the same as authentic sharing
Depression requires professional help, not just willpower
Envy reveals what you want, not what others have taken from you
Obsessions push people away instead of creating connection
The most important relationship is with yourself
If you're recognizing toxic patterns in yourself right now, know that awareness is the first step. Change is possible. Healing takes time, professional support, and deep work on root causes—but it's absolutely possible.
For the complete story of moving from toxic depression to genuine healing and healthy friendships my book provides everything you need.
Get your copy today and start your journey from toxicity to authentic connection.
6 Hard Truths About Social Expectations When You're Autistic
You spent weeks planning it. You invited people who seemed interested. You built up this vision in your head of how it would all unfold—the perfect celebration that would finally prove you belonged, that you had friends, that you were just like everyone else.
Then reality hits. One by one, people cancel. The plans fall apart. You end up alone on what was supposed to be your big night, eating fast food by yourself while everyone else celebrates with their tight-knit friend groups.
For autistic people who struggle with social connections, this pattern is painfully familiar. We hear about how others celebrate milestones and assume we can create the same experience. We mistake polite responses for genuine commitment. We build elaborate fantasies to cope with loneliness, then crash when reality refuses to cooperate.
This is about the hard lessons I learned when my 21st birthday became one of the most humiliating experiences of my college years—and what every autistic person needs to understand about the difference between acquaintances and actual friends.
Table of Contents
Truth #1: Acquaintances Are Not Friends (No Matter How Nice They Seem)
Truth #2: "Common Courtesy" Responses Don't Mean Commitment
Truth #3: Your Fantasy Fills the Gap Where Real Friendships Should Be
Truth #4: You Can't Build a Celebration on Casual Connections
Truth #5: Oversharing With the Wrong People Damages Your Reputation
Truth #6: Desperation Pushes People Away Instead of Drawing Them In
What Actually Builds Real Friendships
Key Takeaways for Managing Expectations
Truth #1: Acquaintances Are Not Friends (No Matter How Nice They Seem)
The Fundamental Mistake
When I planned my 21st birthday celebration, I invited people I barely knew. I had:
Taken one class with Savannah over the summer
Watched TV a handful of times with Tia
Seen various floormates occasionally in the dorm
These were acquaintances at best. But because I was desperate for friends and they'd been polite to me, I convinced myself they were close enough to celebrate my birthday.
Understanding the Difference
Acquaintances:
People you see regularly in shared spaces
Classmates you chat with before or after class
Neighbors you exchange pleasantries with
Colleagues you make small talk with
Friends:
People who actively seek out your company
Individuals you've spent significant one-on-one time with
Those who share personal information reciprocally
People who reach out to you, not just respond when you reach out
Why Autistic People Confuse the Two
Autistic people often struggle to distinguish acquaintances from friends because:
Limited social experience means we lack the pattern recognition that helps neurotypical people gauge relationship depth.
Literal thinking makes us take polite responses at face value rather than reading between the lines.
Desperate for connection causes us to elevate any positive interaction into potential friendship.
Difficulty reading social cues prevents us from noticing when someone is being polite versus genuinely interested.
The Reality Check
Most of the people I invited weren't spending time with me outside of class or casual dorm encounters. They hadn't invited me to their events. They didn't text or call me to hang out.
These weren't friends. They were people who knew my name and were polite when they saw me.
Expecting them to celebrate my birthday was asking for a level of emotional investment they'd never demonstrated.
Truth #2: "Common Courtesy" Responses Don't Mean Commitment
What People Actually Mean
When I told people about my birthday plans over the summer, many said things like:
"That sounds fun!"
"I'd be up for that"
"Yeah, maybe I'll come"
"We'll see what happens"
I took these responses as commitments. They were actually polite ways of saying "maybe" or even "probably not."
The Polite Response Trap
Neurotypical people use vague, noncommittal language as social lubrication. When they say "I'd be up for celebrating," they often mean:
"That's a nice idea but I'm not committing"
"I'll come if I don't have anything better to do"
"I'm being polite but don't actually plan to attend"
"I'm leaving myself an easy out"
What Actual Commitment Sounds Like
Compare those vague responses to what actual commitment looks like:
"Yes, I'll be there! What time should I meet you?"
"I'm definitely coming. Should I invite anyone else?"
"I've marked it on my calendar. Looking forward to it!"
"I'll make sure I'm free that night"
Notice the difference? Real commitment is specific, enthusiastic, and action-oriented.
Why This Matters for Autistic People
Autistic people tend to communicate directly and honestly. When we say we'll do something, we mean it. We assume others operate the same way.
This creates painful misunderstandings when we take polite, non-committal responses as genuine promises.
Sonia's podcast is a must-listen resource for autistic individuals seeking affirming mental health care - tune in here.
Truth #3: Your Fantasy Fills the Gap Where Real Friendships Should Be
Building the Story in Your Head
Throughout the summer, I constructed an elaborate vision of my 21st birthday:
Group dinner at the Italian restaurant downtown
Everyone going to bars together afterward
Celebrating with friends who cared about me
Finally feeling like I "arrived" and belonged
This fantasy became more real to me than actual reality. I replayed it in my mind constantly, adding details, imagining conversations, picturing the whole evening.
Why We Build Fantasies
Fantasy serves important psychological functions when you're lonely:
It provides hope that things will eventually get better and you'll find your people.
It creates temporary relief from the pain of current isolation.
It offers control over an imagined scenario when real relationships feel impossible to build.
It fills the void where genuine connections should exist.
The Danger of Living in Fantasy
The problem with elaborate fantasies is they:
Set unrealistic expectations that reality can't possibly meet.
Prevent you from seeing the actual state of your relationships clearly.
Increase devastation when the fantasy inevitably crumbles.
Distract from building real connections by providing imaginary ones.
The Crash
When the fantasy bubble burst—when people canceled one after another, when Tia said "I'll only come if I feel like it," when Nadia had to work—the emotional crash was severe.
I cried every day the week of my birthday. The anxiety built to the point where I could barely eat. The cortisol in my stomach made me physically ill.
The gap between fantasy and reality was so extreme that it felt like trauma.
Truth #4: You Can't Build a Celebration on Casual Connections
The Foundation Problem
Imagine trying to build a house on sand. No matter how well you design it, the foundation won't support the structure. The same applies to celebrations built on casual acquaintanceships.
What I Did Wrong
I made several critical errors:
I invited people I barely knew to an intimate celebration that requires close friendships.
I assumed their politeness meant closeness when it just meant they had good manners.
I didn't have established patterns of hanging out with these people outside structured activities.
I expected them to prioritize my event when they had no emotional investment in me.
What Milestones Actually Require
Celebrating major milestones like 21st birthdays requires:
Close friends who genuinely care about you
Established relationships with regular contact and reciprocal investment
People who seek you out, not just respond when you reach out
Mutual emotional investment built over time through shared experiences
You can't manufacture this foundation in a few weeks or months of casual contact.
The Alternative Approach
Instead of planning an elaborate celebration with acquaintances, I could have:
Celebrated with family who genuinely cared
Done something meaningful alone or with one close person
Acknowledged I didn't yet have the friend group for the celebration I wanted
Set a goal to build those friendships before the next milestone
This would have been emotionally difficult but far less devastating than watching an elaborate fantasy crumble.
Truth #5: Oversharing With the Wrong People Damages Your Reputation
What I Shared (That I Shouldn't Have)
According to my floormate Ankita, I had damaged my reputation by sharing personal information with people who weren't close friends:
Talking about having a crush on someone who didn't like me back
Mentioning I'd never been kissed
Sharing personal struggles with people I barely knew
Why This Matters
Information you share gets used in ways you can't control:
It becomes gossip that spreads through social networks.
It gives people ammunition to mock or judge you.
It makes others uncomfortable when shared prematurely in relationships.
It signals poor social boundaries, which makes people wary of getting closer.
The Oversharing Trap for Autistic People
Autistic people often overshare because:
We struggle to gauge relationship depth and don't know what's appropriate to share at different stages.
We're honest and straightforward by nature and assume others will be too.
We're desperate to connect and use personal disclosure to create intimacy quickly.
We don't realize information spreads and gets used against us.
What Appropriate Sharing Looks Like
Information should be shared gradually as relationships deepen:
Early stage (acquaintances):
Surface-level topics: classes, weather, general interests
Safe small talk that doesn't reveal vulnerabilities
Developing friendship:
Some personal preferences and opinions
Stories about experiences that don't involve deep emotions
Interests and hobbies in more detail
Close friendship:
Personal struggles and challenges
Romantic interests and rejections
Deeper emotional experiences
Vulnerabilities and insecurities
Sharing deep personal information with acquaintances creates discomfort and damages how people perceive you.
In my book, I provide detailed guidance on what's appropriate to share at different relationship stages and how to recognize when you're oversharing before it damages your reputation further.
Truth #6: Desperation Pushes People Away Instead of Drawing Them In
The Anxiety Spiral
As my birthday approached and people started canceling, my anxiety skyrocketed. I:
Reminded people constantly about the celebration
Felt physically ill from stress and cortisol buildup
Could barely eat or concentrate on anything else
Became increasingly frantic about making the fantasy happen
Why Desperation Repels
Desperation creates discomfort in others because:
It signals neediness that feels overwhelming to people who barely know you.
It creates pressure to fulfill expectations they never agreed to.
It makes them feel guilty for not caring as much as you want them to.
It highlights the imbalance in how you view the relationship versus how they view it.
The Therapist's Warning
My therapist, Dr. Theroux, tried to warn me: "Remember, Sonia, people don't like to keep hearing about the same thing again and again. Do your best to stay in the present."
She recognized I was becoming overeager and overexcited—classic signs of desperation that turn people off.
What Confidence Looks Like Instead
Confidence in social situations means:
Having plans but not being attached to specific people showing up
Being okay if people decline without taking it personally
Not reminding people repeatedly about your event
Having backup plans that don't depend on others' participation
Maintaining emotional stability regardless of who attends
This is incredibly difficult when you're lonely and desperate for connection. But desperation has the opposite effect of what you want—it pushes people away instead of drawing them in.
The Devastating Reality
The day of my 21st birthday, the last pieces fell apart:
Leila wasn't feeling well and couldn't come
Phaedra was eating dinner earlier than I could join
Nadia had to work and was told not to encourage alcohol consumption
Savannah had a mandatory sorority meeting
I ended up alone at a fast-food restaurant eating a fish sandwich and chocolate shake for my birthday dinner.
What Actually Builds Real Friendships
The Brutal Truth I Had to Learn
You can't force friendships into existence by planning elaborate events. Real friendships develop through:
Consistent, low-key contact over extended time periods.
Reciprocal effort where both people initiate and invest equally.
Shared experiences that happen organically, not through forced celebrations.
Gradual deepening of trust and emotional intimacy.
Natural compatibility that can't be manufactured through willpower.
What I Should Have Done Instead
Rather than planning an elaborate 21st birthday with acquaintances, I should have:
Focused on building one or two deeper friendships through regular, consistent contact.
Accepted my current social reality instead of trying to force it to match others' experiences.
Celebrated modestly in ways that matched my actual relationship status.
Used the milestone as motivation to build genuine friendships over the coming year, not as a deadline to manufacture them.
Worked with my therapist on realistic relationship-building strategies instead of fantasy fulfillment.
The Skills I Lacked
Ankita pointed out important skills I needed:
How to help a friend in need - When she hurt her foot and I rushed past to my exam, I should have said: "I'm so sorry you aren't feeling well. Is there anything I can do? I have an exam I need to rush to at the moment."
Understanding boundaries - Both my own and others', recognizing what's appropriate to share and when.
Standing up for myself - Which I was learning with Janet but needed to extend to other relationships.
Reading social situations - Understanding when someone is genuinely interested versus being polite.
These skills can't be learned overnight. They require practice, feedback, and often professional guidance.
Key Takeaways for Managing Expectations
Adjust Expectations to Match Reality
The most painful part of my 21st birthday wasn't being alone—it was the enormous gap between what I expected and what happened.
If I'd recognized that I had acquaintances, not friends, I could have:
Celebrated with family instead
Had modest plans that matched my social reality
Avoided the devastating crash when fantasy met reality
Quality Matters More Than Quantity
Stop measuring social success by:
Size of celebration
Number of people who attend your events
How your milestones compare to others' experiences
Start measuring it by:
Depth of a few genuine connections
Reciprocal investment in relationships
Quality of interactions, not quantity
Build Friendships Before Planning Celebrations
Celebrations are the result of established friendships, not the catalyst for creating them.
Before planning group events, ask:
Do these people regularly spend time with me outside structured settings?
Have they invited me to their events?
Is there reciprocal effort in maintaining contact?
Would they notice if I disappeared from their lives?
If the answers are no, you're dealing with acquaintances who won't show up for celebrations.
Learn From Each Painful Experience
My 21st birthday was humiliating. Eating that fish sandwich alone while imagining others celebrating with their friend groups felt like rock bottom.
But it taught me critical lessons:
Fantasy doesn't create reality
Desperation pushes people away
You can't force friendships on your timeline
Acquaintances won't show up like friends do
These lessons, painful as they were, eventually helped me build genuine friendships by adjusting my approach.
Protect Yourself From Repeated Devastation
If you keep experiencing this pattern:
Work with a therapist on realistic relationship-building
Learn to distinguish polite responses from actual commitments
Stop building elaborate fantasies to cope with loneliness
Focus on one or two potential friends at a time
Accept that building genuine friendships takes years, not weeks
Ready to learn the complete story of my 21st birthday disaster and what I eventually learned about building real friendships instead of manufacturing fake ones? My book provides the full account, get your copy today.
Moving Forward
The night didn't end with the fish sandwich. I eventually went to the bar where my roommate was celebrating with her friends. I got lost in the sensory overload—the lights, the music, the crowds. My roommate kept telling me to drink more. I wanted to forget the harsh reality through alcohol.
I heard the DJ announce other people's birthdays over the stereo. Each announcement felt like a bee sting—a reminder that other people had the tight friend groups celebrating them that I desperately wanted but didn't have.
That night crystallized a brutal truth: you can't drink away loneliness. You can't force friendships through elaborate planning. You can't manufacture belonging through sheer determination.
What you can do is learn from the devastation, adjust your approach, and slowly build the genuine connections that eventually replace the fantasy.
For the complete journey from devastating birthday disasters to eventually building real friendships—including all the mistakes I made, lessons I learned, and strategies that actually worked—my book provides everything you need to stop repeating this painful pattern.
Get your copy today and learn how to build realistic expectations that protect you from crushing disappointment.