

Autism and Time Management: Practical Strategies for Adults
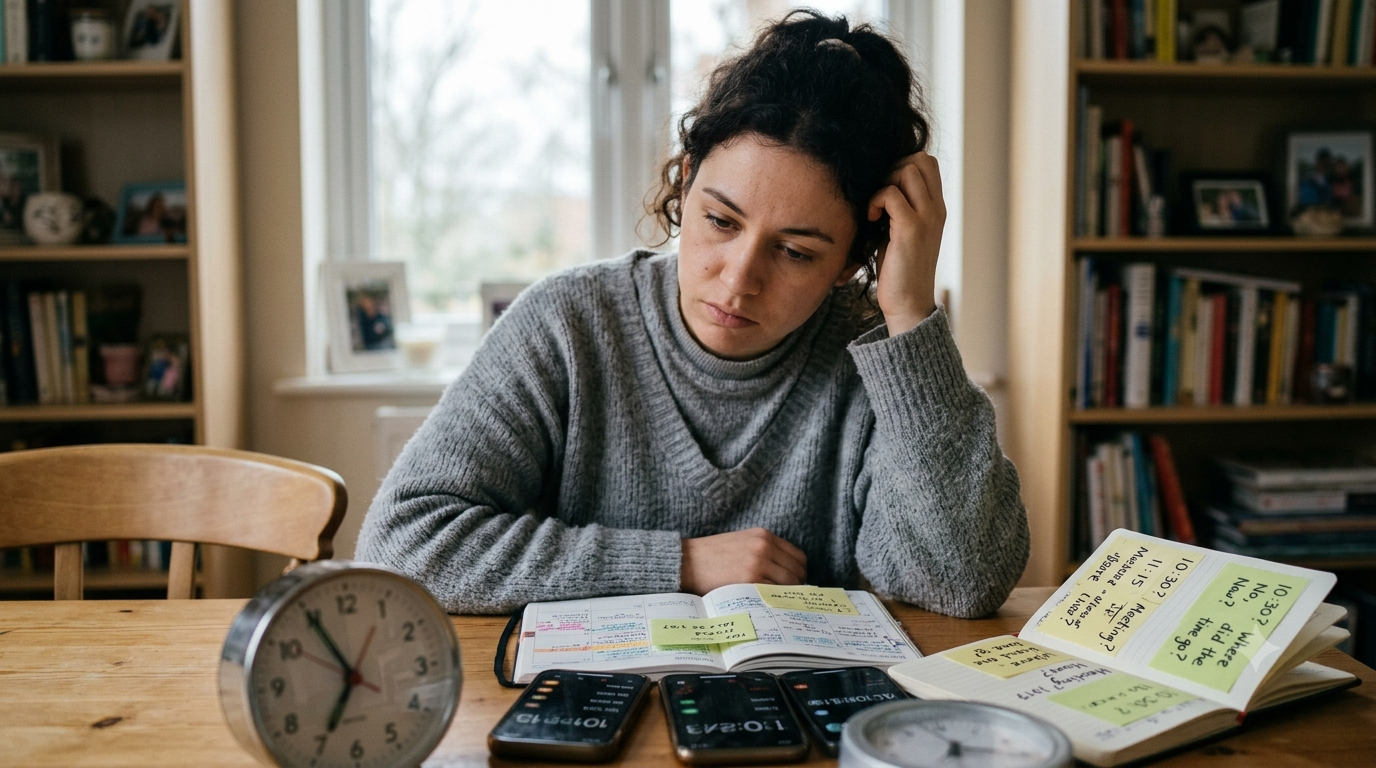
Autism and time management is one of the most quietly debilitating combinations that autistic adults navigate every single day. If you are perpetually late despite genuinely trying not to be, if time seems to disappear without warning, if transitions between tasks feel like trying to change direction while running at full speed, and if the gap between what you intended to do today and what you actually managed to do feels humiliating rather than simply inconvenient, this post is written for you.
Autism and time management difficulties are not a character flaw. They are not laziness, poor prioritization, or a lack of caring about the people and commitments in your life. They are the direct result of neurological differences in how the autistic brain processes time, transitions, and executive functioning, and understanding that distinction is the first and most important step toward actually building strategies that work.
Table of Contents
Why Autism and Time Management Is So Hard: The Neurology
Time Blindness and Autism
Transitions and Task Switching in Autism
Hyperfocus and Time Management in Autism
Executive Functioning and Autism Time Management
The Emotional Weight of Autism and Time Management
Practical Strategies for Autism and Time Management
Technology Tools That Help
Workplace Strategies for Autism and Time Management
FAQs
Final Thoughts
References
Why Autism and Time Management Is So Hard: The Neurology
Autism and time management difficulties do not come from the same place as typical time management struggles. Most time management advice is built around motivational strategies, prioritization frameworks, and productivity systems. These assume that the person can sense time passing, can switch between tasks with reasonable fluidity, and has executive functioning systems that work well enough to be organized with the right tools.
For many autistic adults, none of those assumptions hold. The neurological differences underlying autism affect time perception, task switching, planning, initiation, and working memory in ways that make standard time management advice either unhelpful or actively counterproductive.
Understanding the specific neurological mechanisms driving autism and time management difficulties is what allows genuinely useful strategies to be built, because the right strategy for a neurological problem looks completely different from the right strategy for a motivational one.
Time Blindness and Autism
Time blindness is one of the most significant contributors to autism and time management difficulties and one of the least understood by the people around autistic adults.
Time blindness is exactly what it sounds like: an inability to accurately perceive the passage of time in the moment. It is most commonly associated with ADHD, which frequently co-occurs with autism, but it is also a feature of autistic neurology independently.
For autistic adults with time blindness, there are effectively only two time zones: now and not now. Something is happening right now, or it is in an undifferentiated future that does not yet feel real or urgent. The appointment in two hours does not feel two hours away. It feels like something in the abstract future until suddenly it is happening and there was no subjective experience of the time between.
This is why autistic adults can look up from a task and genuinely not understand where three hours went. The time passed. They simply did not experience it in a way that allowed them to track it. Time blindness in autism and time management is not an excuse. It is an accurate description of a neurological experience that is as real and as involuntary as any other autistic trait.
Research has consistently identified time blindness as a feature of neurodevelopmental conditions including ADHD and autism, driven by differences in working memory and the brain's internal timing systems.
The Emotional Weight of Autism and Time Management
Before getting into strategies, the emotional dimension of autism and time management deserves honest acknowledgment because it is real and it is significant.
Autistic adults who struggle with time management carry a disproportionate load of shame around it. They have been late to important things. They have missed deadlines that mattered. They have disappointed people they care about, not because they did not care but because their neurology did not cooperate with their intentions. And they have received the message, repeatedly and from many directions, that this is a personal failing rather than a neurological reality.
That accumulated shame is not just emotionally painful. It actively interferes with time management itself, because shame and self-blame consume cognitive and emotional resources that could otherwise go toward building and maintaining the external systems that actually help.
The right starting point for autism and time management is therefore self-compassion, not as a platitude but as a practical prerequisite. You are not failing at something everyone else finds easy. You are navigating a genuine neurological challenge with inadequate tools, and what you need is better tools, not more self-criticism.
For autistic adults who are carrying years of accumulated shame around executive functioning and daily life management, Sonia's self-esteem coaching is built for exactly that work.
Book a self-esteem coaching session with Sonia here and start replacing the shame narrative with an accurate one that actually helps you move forward.
Transitions and Task Switching in Autism
If time blindness explains why time disappears, the autistic difficulty with transitions and task switching explains why autism and time management creates so many missed deadlines and incomplete sequences of activity.
Autistic brains are generally very good at deep focus within a single task and significantly less good at moving between tasks on demand. The neural cost of switching from one activity to another is higher for many autistic individuals than for neurotypical peers, requiring genuine cognitive effort and time to disengage from one thing and reorient to another.
This is why an autistic adult who needs to stop what they are doing and leave the house in fifteen minutes may still be in the same spot an hour later. It is not that they did not hear you. It is that the cognitive and neurological work of disengaging from what they are doing, reorienting to the new demand, and initiating the sequence of actions required to leave is genuinely effortful in a way that does not resolve simply by being told it needs to happen sooner.
Autism and time management therefore requires transition support built into daily structure rather than relying on the autistic person to manage the cognitive switching demand purely through willpower.

Hyperfocus and Time Management in Autism
Hyperfocus is one of the most distinctive features of autistic and ADHD neurology and it has a direct and significant relationship with autism and time management.
Hyperfocus is the state of complete absorption in a task or interest where external awareness, including awareness of time, drops away almost entirely. For autistic adults, hyperfocus tends to occur around special interests and engaging tasks, and it produces a quality of focus and output that is genuinely extraordinary. It also produces a complete inability to track or respond to time during the hyperfocus period.
The same neurology that makes hyperfocus possible also makes it very difficult to exit on demand. An autistic adult in hyperfocus who needs to stop and do something else is not ignoring the need. They are genuinely struggling to access the cognitive machinery required to disengage and redirect.
Managing hyperfocus is therefore one of the central practical challenges of autism and time management, and the strategies that help are almost entirely external rather than internal. The autistic adult cannot simply decide to exit hyperfocus more easily. They can build external systems that interrupt and signal from outside the hyperfocus state.
Executive Functioning and Autism Time Management
What is sometimes described as autism and time management is often more accurately described as autism and executive functioning, because executive functioning is the umbrella system that time management depends on.
Executive functioning includes planning, organizing, initiating, monitoring, shifting, and completing tasks. It involves the ability to hold a goal in mind while completing the steps toward it, to prioritize competing demands, to initiate action without external prompting, and to monitor progress against a plan in real time.
Many autistic adults experience significant executive functioning differences that affect all of these capacities to varying degrees. The result is not that they are incapable of doing what needs to be done. It is that the internal cognitive scaffolding that most people use to organize and sequence their day does not work reliably without external support.
This is why autism and time management improves dramatically with external systems, structures, and tools, not because autistic adults need to be managed but because external scaffolding provides what the internal executive functioning system cannot reliably supply on its own.
Dropped in a Maze by Sonia Chand addresses the experience of navigating daily life with autistic neurology, including the executive functioning challenges that make time management so hard, with the honest, practical perspective that comes from having lived it rather than simply studied it.
Practical Strategies for Autism and Time Management
Here is what the evidence and lived experience of autistic adults consistently supports as genuinely effective for autism and time management:
Make time visible
Because time blindness means internal time perception is unreliable, making time externally visible is one of the most effective strategies available. Time timer clocks, which show time as a visual representation of a shrinking segment rather than as digits, are widely used and highly effective. Analog clocks showing the current position in the day provide a more intuitive sense of time passing than digital displays.
Build transition warnings into every schedule
Rather than requiring the task switch to happen immediately, build in explicit transition warnings. A timer set fifteen minutes before a required transition gives the autistic nervous system time to begin the disengagement process before the actual switch is required.
Use time blocking rather than to do lists
Open-ended to do lists are poorly suited to autistic time management because they do not specify when things will happen. Time blocking, assigning specific tasks to specific time blocks in the day, externalizes the planning function and removes the need to make real-time decisions about what to do next throughout the day.
Build transition buffers
When calculating how long something will take, build in deliberate transition buffer time between activities. Autistic adults consistently underestimate transition time and overestimate how much can be done in a given period. Deliberate buffering compensates for this.
Start earlier than feels necessary
Because the autistic experience of time means that future events do not feel real until they are imminent, building a rule of starting preparation significantly earlier than feels necessary compensates for the experiential gap between two hours away and now.
Use body doubling
Body doubling, working alongside another person whether in person or virtually, is one of the most effective executive functioning supports for both autistic and ADHD adults. The presence of another person provides an external regulatory anchor that helps maintain task engagement and reduces the likelihood of losing time to hyperfocus or executive functioning failure.
Technology Tools That Help
Several technology tools are particularly well suited to the specific challenges of autism and time management:
Time timer apps including the Time Timer app provide visual representations of time passing that address time blindness directly.
Google Calendar with notifications set to go off thirty minutes, fifteen minutes, and five minutes before any appointment or transition provides layered external reminders that compensate for the internal timing system.
Structured planning apps including Structured and Tiimo are specifically designed for neurodivergent adults and provide visual daily schedules that time block activities in a format that works with autistic processing rather than against it.
Task management apps including Todoist and Things can help with the planning and organizing functions of executive functioning when used with time-based reminders attached to every task rather than open-ended lists.
Workplace Strategies for Autism and Time Management
Autism and time management in the workplace deserves specific attention because the consequences of time management difficulties at work can be significant and because the workplace is one of the environments where autistic adults are least likely to have received accommodation for executive functioning differences.
Workplace strategies that specifically address autism and time management include:
Requesting written schedules and agendas in advance of meetings and work periods so the day's structure is externally visible rather than requiring ongoing planning.
Asking for deadlines to be broken into intermediate milestones rather than single end dates, which provides external checkpoints that compensate for the difficulty of self-monitoring progress over extended time periods.
Using calendar blocking for all work tasks including deep work periods, so that the entire workday is externally structured and the decision of what to do next never needs to be made in real time.
Disclosing executive functioning differences where safe and appropriate to do so in order to request reasonable accommodations including flexible scheduling, written instructions, and structured check-ins.
For autistic adults who want support building workplace strategies that genuinely accommodate their neurology, Sonia's socio-emotional coaching provides exactly that kind of practical, personalized guidance.
Book a coaching session with Sonia here and start building the workplace strategies that work with your autistic brain rather than against it.
FAQs
Why is autism and time management so difficult?
Neurological differences in time perception, task switching, working memory, and executive functioning mean that internal time management systems do not work reliably for many autistic adults without external support.
What is time blindness in autism?
Time blindness is the inability to accurately perceive the passage of time in the moment, resulting in time appearing to disappear without warning and future events not feeling real until they are imminent.
Can autistic adults improve their time management?
Yes, significantly, through external systems, tools, and structures that compensate for the internal executive functioning differences rather than trying to fix those differences through willpower.
What is the most effective tool for autism and time management?
Visual time representation tools that make time passing externally visible, combined with structured time blocking and layered transition warnings, are consistently the most effective combination.
Is time management difficulty in autism related to ADHD?
Many autistic adults also have ADHD, and the two conditions share executive functioning and time perception challenges. However, time management difficulties are also present in autistic adults without ADHD.
Should I disclose my autism at work to get time management support?
Disclosure is a personal decision. Where it is safe to do so, disclosing executive functioning differences and requesting specific accommodations can significantly improve workplace time management outcomes.
Final Thoughts
Autism and time management is hard in ways that standard productivity advice does not address, cannot address, because it is built for a neurological system that works differently from the one you have.
The path forward is not trying harder with the same tools that have not worked. It is building external systems that work with your specific neurology, understanding what is actually driving the difficulty, and releasing the shame that has accumulated around something that was never a character flaw in the first place.
You are not bad at time. You have a brain that experiences time differently. And that brain, with the right tools around it, is entirely capable of building a life that works.
References:
Autism Speaks. Autism and time management [Internet]. Available from:https://www.autismspeaks.org/expert-opinion/autism-time-management
Colorosa S. Autism Time Management: How to Approach It [Internet]. Autism Parenting Magazine; 2025 Jan 6. Available from:https://www.autismparentingmagazine.com/autism-time-management/
Casassus M, Poliakoff E, Gowen E, Poole D, Jones LA. Time perception and autistic spectrum condition: A systematic review. Autism Res. 2019;12(10):1440-1462. Available from:https://pmc.ncbi.nlm.nih.gov/articles/PMC6852160/

Autism and Picky Eating: What Is Behind It and What Helps
Autism and picky eating is one of the most exhausting and least understood challenges that autism families face at the dinner table every single day. If your autistic child will only eat five foods, rejects anything new without even trying it, or has complete meltdowns over textures, colors, or foods touching each other on the plate, you are not dealing with a spoiled child or a parenting failure. You are dealing with a genuine neurological reality that most advice about picky eating completely misses.
Autism and picky eating go together far more often than most people realize. Research suggests that feeding difficulties affect between 46 and 89 percent of autistic children, making it one of the most prevalent co-occurring challenges in the entire autism population. Understanding what is actually driving it, beneath the surface of the refused plate and the mealtime meltdown, changes everything about how you respond to it.
This post covers what autism and picky eating actually involves neurologically, what the research says about causes and effective approaches, and what genuinely helps at home without making mealtimes a battleground.
Table of Contents
Autism and Picky Eating
Sensory Processing and Autism Picky Eating
Neophobia and the Fear of New Foods
Routine and Rigidity in Autism and Picky Eating
Gastrointestinal Issues and Autism Picky Eating
The Pressure Problem: Why Forcing Does Not Work
What Actually Helps With Autism and Picky Eating
Food Chaining: A Practical Strategy
When to Seek Professional Support
Nutrition Concerns in Autism and Picky Eating
FAQs
Final Thoughts
References
Autism and Picky Eating
The first and most important thing to understand about autism and picky eating is that it is categorically different from typical childhood fussiness.
Typical picky eating in neurotypical children tends to peak around age two and gradually reduce as children are repeatedly exposed to a wider variety of foods. It is developmentally normal, it is generally not nutritionally serious, and it usually resolves with time and patient exposure.
Autism and picky eating does not follow this pattern. It tends to be more extreme, more persistent, and more resistant to the standard advice about repeated exposure and family meals. The foods accepted by autistic children who are picky eaters are often severely limited in variety, sometimes to fewer than ten foods. The rejection of new foods is often immediate, visceral, and accompanied by genuine distress rather than mild reluctance. And the preferences, once established, tend to be extremely specific, not just chicken but that brand of chicken nugget, cooked for that length of time, served on that plate.
This level of specificity and rigidity is not stubbornness. It is the autistic nervous system communicating that food is a genuinely complex sensory and regulatory experience that requires very specific conditions to feel safe.

Sensory Processing and Autism Picky Eating
Sensory processing is at the heart of autism and picky eating, and understanding this changes the entire frame through which you view the refused meal.
Food is one of the most sensorially complex experiences humans encounter. A single bite involves texture, temperature, taste, smell, visual appearance, and the sound it makes when chewed. For neurotypical people, the brain filters and integrates all of these inputs automatically and simultaneously, producing an overall eating experience that is manageable and often pleasant.
For many autistic children, the sensory filtering that makes eating manageable is not working the same way. Individual sensory channels may be significantly more sensitive than typical. A texture that is mildly unpleasant to a neurotypical child can be genuinely intolerable to an autistic one, producing a gag response, physical distress, or a full meltdown not because the child is being dramatic but because their nervous system is genuinely registering the experience as unbearable.
Common sensory triggers in autism and picky eating include:
Texture, particularly mixed textures, mushy textures, or unexpected texture changes
Temperature, with many autistic children strongly preferring foods within a very specific temperature range
Smell, which is processed before food is even tasted and can make an otherwise acceptable food impossible to eat
Visual appearance, including color, shape, and the arrangement of food on the plate
Sound, including the sound of food being chewed or the sounds in the eating environment
Understanding which specific sensory channels are driving your child's food refusal is the starting point for any effective intervention.
Neophobia and the Fear of New Foods
Alongside sensory processing, food neophobia, the fear of new or unfamiliar foods, is a significant driver of autism and picky eating that is worth understanding separately.
Food neophobia exists on a spectrum in the general population but is significantly more common and more intense in autistic children. The autistic brain's strong preference for predictability and sameness, which is helpful and protective in many contexts, applies to food as much as to any other domain of life.
A familiar food is safe because its sensory properties are known and predictable. A new food carries the risk of an unknown and potentially overwhelming sensory experience. Refusal of new foods is therefore not irrationality. It is a sensible risk-management response by a brain that has learned to prioritize predictability over novelty.
This understanding is important because it reframes the question of how to introduce new foods. The goal is not to convince the child that the new food is good. The goal is to make the new food feel safe and predictable before any pressure to eat it is introduced.
The On the Spectrum podcast with Sonia Chand covers these kinds of practical, real-world autism challenges in honest conversations that go beyond theory and into what actually makes a difference for families.
Routine and Rigidity in Autism and Picky Eating
The autistic need for routine and sameness contributes to autism and picky eating in ways that extend beyond pure sensory sensitivity.
For many autistic children, the specific way a food is prepared, presented, and served is as important as the food itself. The brand, the packaging, the plate, the order in which foods are eaten, whether foods are touching each other, and the physical environment of the meal can all be part of the rigid pattern that defines safe eating.
When any of these elements changes unexpectedly, the food that was previously accepted can become impossible to eat, not because the food itself has changed but because the predictable pattern around it has been disrupted.
This is not manipulation or attention seeking. It is the autistic nervous system responding to an unexpected change in a domain where predictability is essential for safety.
Recognizing this helps parents understand why a previously accepted food can suddenly be rejected after a packaging change, a different preparation method, or even a meal served in a different room. The food has not become worse. The unpredictability has become intolerable.
Gastrointestinal Issues and Autism Picky Eating
One contributing factor to autism and picky eating that is frequently missed is the higher rate of gastrointestinal issues in autistic individuals.
Research consistently shows that gastrointestinal problems including constipation, reflux, and gut motility issues affect autistic individuals at significantly higher rates than the general population. When eating is associated with physical discomfort or pain, food avoidance is a rational protective response rather than a behavioral problem.
If your child's autism and picky eating is particularly severe or is accompanied by behavioral distress around mealtimes that seems disproportionate to the sensory explanation, a gastrointestinal evaluation with a pediatrician or pediatric gastroenterologist is a worthwhile step before focusing exclusively on behavioral or sensory interventions.
The Pressure Problem: Why Forcing Does Not Work
One of the most important things to understand about autism and picky eating is that pressure, whether explicit or subtle, consistently makes the situation worse rather than better.
Research on feeding in both autistic and neurotypical populations consistently shows that pressure around eating, including requiring a child to try a food before leaving the table, offering rewards for eating new foods, or expressing negative emotion around food refusal, is associated with increased food avoidance and increased mealtime distress.
For autistic children, the pressure problem is amplified significantly. A nervous system that is already primed to detect threat responds to feeding pressure by associating the pressured food, and sometimes the entire mealtime, with threat and distress. This makes the food harder to accept in the future, not easier.
The approach that actually works is the opposite of pressure. It is low demand, high safety, and very gradual exposure without any requirement to eat.
For families who are also navigating a demand avoidance profile alongside autism and picky eating, the post on pathological demand avoidance in autism covers the specific dynamics of demand-driven anxiety that can make mealtimes particularly challenging and what approaches genuinely reduce it.
What Actually Helps With Autism and Picky Eating
Here is what the evidence and clinical experience consistently supports as effective for autism and picky eating:
Create a calm, predictable mealtime environment
Reduce sensory load at the table. Consider lighting, background noise, and seating. Keep the mealtime structure consistent and predictable. Consistency is safety.
Remove all pressure to eat
Make the table a no-pressure zone. Food is offered, not required. The child decides what and how much they eat from what is offered. This is called a division of responsibility and it is supported by significant research in pediatric feeding.
Respect the sensory experience
Do not minimize, dismiss, or challenge the child's reported sensory experience of food. If they say it feels wrong, it feels wrong to them. Validating that experience is the foundation of any trust-based feeding approach.
Serve accepted foods alongside new ones
Always include at least one accepted food at every meal. The presence of a safe food reduces the anxiety of encountering something unfamiliar and creates the conditions for gradual exposure without distress.
Use food chaining for expansion
See the next section for a full explanation of this approach.
Involve the child in food preparation
Children who participate in preparing food develop familiarity with it before it reaches their plate. This gradual, sensory exposure without eating pressure is one of the most effective routes to food acceptance.

Food Chaining
Food Chaining: A Practical Strategy
Food chaining is one of the most evidence-based approaches for expanding the food repertoire of autistic children with significant picky eating, and it is worth understanding in detail.
Food chaining works by identifying the specific properties of accepted foods and using those properties as a bridge to gradually introduce new foods. Rather than presenting an entirely new food cold, food chaining moves in very small steps from what is accepted toward what is new, changing only one variable at a time.
For example: if a child accepts plain salted crackers, the chain might move to a slightly different brand of salted cracker, then to a cracker with a slightly different texture, then to a different crunchy food with a similar shape, then to something with a similar shape and a very mild flavor addition.
Each step changes only one property at a time. The child's nervous system encounters novelty in the smallest possible dose, which keeps the threat response from activating and allows genuine familiarity to develop.
Research has supported food chaining as an effective approach for expanding food acceptance in children with significant food selectivity, with gains maintained over follow-up periods.
Dropped in a Maze by Sonia Chand speaks to the experience of navigating the practical daily challenges of autism parenting, including the food battles, the mealtime meltdowns, and the exhausting search for what actually works, with the kind of honest, grounded wisdom that only comes from having lived it.
When to Seek Professional Support
Autism and picky eating that is affecting your child's nutritional status, growth, or quality of life warrants professional support beyond what general parenting strategies can provide.
Seek professional support when:
Your child is eating fewer than fifteen to twenty foods total
You have concerns about nutritional deficiencies or growth
Mealtimes are causing significant and consistent distress for your child or your family
The food repertoire is shrinking over time rather than staying stable or expanding
You suspect gastrointestinal issues are contributing to the problem
The professionals best equipped to help with autism and picky eating include occupational therapists with feeding specialization, speech and language therapists with pediatric feeding experience, pediatric dietitians who understand autism-specific nutritional needs, and feeding therapy programs that use sensory-based rather than pressure-based approaches.
Nutrition Concerns in Autism and Picky Eating
Because autism and picky eating so frequently results in limited food variety, nutritional adequacy is a genuine and important concern that deserves honest attention.
Common nutritional gaps in autistic children with significant picky eating include calcium, vitamin D, zinc, iron, and omega-3 fatty acids. A pediatric dietitian can assess your child's specific intake and recommend appropriate supplementation where genuine deficiencies exist.
A word of caution: the internet is full of specific dietary protocols marketed for autism including gluten-free, casein-free, and ketogenic diets. The evidence for these diets as treatments for autism itself is not strong and some carry nutritional risks when applied to children with already limited food repertoires. Always consult a qualified dietitian before implementing a significant dietary restriction in a child who is already a highly selective eater.
For more on how autism affects the whole child including physical health, the post onwhat are the management of autism covers the full picture of evidence-based approaches including medical management of co-occurring conditions.
FAQs
Why is autism and picky eating so common?
Sensory processing differences, food neophobia, need for routine and sameness, and higher rates of gastrointestinal issues all contribute to the significantly higher rates of picky eating in autistic children.
Is autism picky eating just a phase?
Unlike typical childhood picky eating, autism and picky eating tends to be more persistent and more severe and generally does not resolve on its own without specific intervention.
Does forcing an autistic child to try new foods help?
No. Pressure consistently makes autism and picky eating worse by associating food with threat and distress.
What is food chaining?
Food chaining is an evidence-based approach that uses the properties of accepted foods as a bridge to gradually introduce new foods, changing only one variable at a time.
Should I be worried about nutrition with an autistic picky eater?
Nutritional assessment by a pediatric dietitian is worthwhile if your child eats a very limited variety of foods, as deficiencies in calcium, vitamin D, zinc, and other nutrients are common.
When should I seek professional help for autism and picky eating?
When your child eats fewer than fifteen to twenty foods, when the repertoire is shrinking, when mealtimes are causing significant distress, or when you have concerns about growth and nutrition.
Final Thoughts
Autism and picky eating is not a parenting problem. It is not a behavioral problem. It is a neurological reality that requires neurologically informed responses, not pressure, not rewards for eating, and not the well-meaning but unhelpful advice to just keep offering the food.
When you understand what is actually driving the food refusal, the sensory overload, the neophobia, the need for sameness, and sometimes the physical discomfort, the path forward becomes much clearer. It is slower than you would like. It requires more patience than feels fair. But it is a path that actually leads somewhere, and it starts with understanding your child's experience as genuinely and accurately as you possibly can.
References
Cole L. Autism and food aversions: 7 Ways to help a picky eater [Internet]. Autism Speaks. Available from:https://www.autismspeaks.org/expert-opinion/autism-and-food-aversions
Coleman B. The Difference Between Picky Eating & Problem Feeding for Kids on the Autism Spectrum [Internet]. Autism Dietitian; 2025 Dec 3 (updated 2025 Jul). Available from:https://www.autismdietitian.com/blog/picky-eating-problem-feeding
Mirizzi P, Esposito M, Ricciardi O, Bove D, Fadda R, Caffò AO, Mazza M, Valenti M. Food Selectivity in Children with Autism Spectrum Disorder and in Typically Developing Peers: Sensory Processing, Parental Practices, and Gastrointestinal Symptoms. Nutrients. 2025;17(17):2798. Available from:https://www.mdpi.com/2072-6643/17/17/2798
Białek-Dratwa A, Szczepańska E, Szymańska D, Grajek M, Krupa-Kotara K, Kowalski O. Neophobia—A Natural Developmental Stage or Feeding Difficulties for Children? Nutrients. 2022;14(7):1521. Available from:https://pmc.ncbi.nlm.nih.gov/articles/PMC9002550/
Madra M, Ringel R, Margolis KG. Gastrointestinal Issues and Autism Spectrum Disorder. Child Adolesc Psychiatr Clin N Am. 2020;29(3):501-513. Available from:https://pmc.ncbi.nlm.nih.gov/articles/PMC8608248/
Rommel N, De Meyer AM, Feenstra L, Veereman-Wauters G. Food Chaining: A Systematic Approach for the Treatment of Children With Feeding Aversion. Nutr Clin Pract. 2003;18(3):213-220. Available from:https://www.researchgate.net/publication/7222254_Food_Chaining_A_Systematic_Approach_for_the_Treatment_of_Children_With_Feeding_Aversion

Autism Meltdowns vs Shutdowns: What Is the Difference and How to Handle Both
Autism meltdowns vs shutdowns is one of those topics that every autism family and many autistic adults need to understand deeply, because getting the response wrong in either situation does not just fail to help. It can make things significantly worse and leave lasting damage to the relationship between the autistic person and the people trying to support them.
Autism meltdowns vs shutdowns look different on the surface, feel different from the inside, and require different responses from the people around the autistic person. Understanding that difference is one of the most practical and most immediately useful things a parent or autistic adult can learn, because these experiences are not occasional. For many autistic individuals they are a regular part of life, and how they are handled determines whether the autistic person recovers quickly or carries the weight of the experience for hours or days afterward.
This post covers what autism meltdowns vs shutdowns actually are, what drives them, how to tell them apart, and what genuinely helps in each situation.
Table of Contents
Autism Meltdowns vs Shutdowns: The Core Difference
What Is an Autism Meltdown
What Is an Autism Shutdown
Autism Meltdowns vs Shutdowns: Side by Side
What Causes Autism Meltdowns and Shutdowns
The Warning Signs Before a Meltdown or Shutdown
How to Handle an Autism Meltdown
How to Handle an Autism Shutdown
What Not to Do During Autism Meltdowns vs Shutdowns
After the Meltdown or Shutdown: Recovery
Preventing Autism Meltdowns and Shutdowns
FAQs
Final Thoughts
References
Autism Meltdowns vs Shutdowns: The Core Difference
Autism meltdowns vs shutdowns both happen when an autistic person's nervous system has been pushed beyond its capacity to cope. They share the same underlying cause, which is neurological overload, but they express that overload in completely opposite directions.
A meltdown is an outward expression of that overload. The nervous system activates the fight or flight response and the result is visible, audible, and often intense. Crying, screaming, hitting, throwing, running, or any combination of these behaviors are the external expression of an internal experience that has exceeded the person's capacity to contain.
A shutdown is an inward expression of the same overload. The nervous system activates the freeze response and the person becomes quiet, still, withdrawn, and unresponsive. From the outside a shutdown can look like sulking, ignoring, or deliberate non-compliance. From the inside it is a state of genuine neurological shutdown where the capacity for speech, social engagement, and sometimes even movement is temporarily inaccessible.
Autism meltdowns vs shutdowns are not choices. Neither is a behavior strategy, a manipulation tactic, or a temper tantrum. Both are involuntary neurological responses to overload that the autistic person is not controlling and cannot simply decide to stop.
What Is an Autism Meltdown
An autism meltdown is an intense, involuntary response to overwhelming sensory, emotional, or cognitive input that exceeds the autistic person's capacity to regulate.
During a meltdown the autistic person is genuinely not in control of what is happening. The prefrontal cortex, which is responsible for reasoning, impulse control, and decision making, is effectively offline. The amygdala, the brain's threat detection system, has taken over. What looks like dramatic or attention-seeking behavior from the outside is the autistic person's nervous system in full crisis mode.
Meltdowns can look like:
Intense crying that cannot be stopped or explained
Screaming or vocalizing loudly
Physical aggression including hitting, biting, or throwing objects
Running or bolting from the situation
Rocking, stimming intensely, or engaging in self-injurious behavior
Complete loss of verbal communication mid-meltdown even in people who are typically verbal
Meltdowns are exhausting. For the autistic person they are physically and emotionally depleting in a way that takes significant time to recover from. The shame and distress that often follows a meltdown, particularly in older children and adults who are aware of how they appeared during it, can be as damaging as the meltdown itself.
What Is an Autism Shutdown
An autism shutdown is the quieter, less visible counterpart to a meltdown, and it is frequently misread entirely because it does not look like distress from the outside.
During a shutdown the autistic person withdraws. They become quiet, still, and unresponsive. Speech may reduce or disappear entirely. Eye contact drops. The person may appear to be ignoring what is said to them, staring blankly, or simply sitting or lying very still.
Shutdowns can look like:
Going completely quiet in the middle of a conversation or activity
Losing the ability to speak even in people who are typically very verbal
Becoming physically still and unresponsive to the environment
Withdrawing to a quiet space and being unable to engage for an extended period
Appearing to be deliberately ignoring people around them
Loss of facial expression and emotional responsiveness
What is happening internally during a shutdown is not peace or indifference. It is the nervous system's freeze response, a protective state that the brain activates when the fight or flight responses are not available or have not worked. The person is not choosing to shut down. Their nervous system has made that choice for them as a self-protective response to overload.
Autism Meltdowns vs Shutdowns: Side by Side
Putting autism meltdowns vs shutdowns directly next to each other makes the distinction clearer:
External appearance: Meltdowns are loud, visible, and often physically intense. Shutdowns are quiet, still, and visually easy to miss.
Nervous system state: Meltdowns are a fight or flight response. Shutdowns are a freeze response.
Verbal communication: During meltdowns verbal communication may become incoherent, repetitive, or shouted. During shutdowns verbal communication often reduces dramatically or disappears.
Common misreading: Meltdowns are often read as tantrums, defiance, or attention seeking. Shutdowns are often read as sulking, ignoring, or deliberate non-compliance.
What makes it worse: Both are worsened by increased pressure, demands, or attempts to talk the person through it in the moment.
What helps: Both require reduction of sensory and social demands, calm presence, and time.
How to Handle an Autism Meltdown
What to do during an autism meltdown is one of the most urgent practical questions for parents and caregivers, and the most important answer is also the most counterintuitive: do less, not more.
During a meltdown:
Reduce sensory input immediately. Lower lights, reduce noise, create physical space.
Remove demands and expectations completely. This is not the moment for reasoning, consequences, or instruction.
Stay calm and speak minimally. A calm regulated nervous system nearby provides co-regulation support even when direct communication is not possible.
Ensure physical safety without restraining unless there is genuine immediate danger.
Do not try to talk the person through it, explain why this is not appropriate, or discuss what happened. The prefrontal cortex is offline. This conversation cannot happen right now.
Wait. Meltdowns end when the nervous system has discharged enough of the overload to begin returning toward regulation.
What the meltdown needs most is time, safety, and a reduction in the inputs that caused the overload in the first place.
How to Handle an Autism Shutdown
Handling an autism shutdown requires a different approach from meltdowns, primarily because the person in a shutdown needs quiet, space, and freedom from expectation rather than any kind of active intervention.
During a shutdown:
Do not push for verbal communication. The person may genuinely not be able to speak and trying to force it increases the distress.
Reduce all demands including social demands like eye contact and responsiveness.
Offer quiet, low-stimulation space without requiring the person to move if they cannot.
Let them know you are nearby and not demanding anything. A simple calm statement like I am here, there is no rush is enough.
Do not interpret the shutdown as anger, sulking, or deliberate ignoring. It is a neurological state, not a social choice.
Give it time. Shutdowns lift when the nervous system has had adequate recovery time and the overload has reduced.
For autistic adults navigating both meltdowns and shutdowns in professional and personal settings, having support that genuinely understands these experiences and can help build practical strategies around them makes an enormous difference.
Book a coaching session with Sonia here and start building the self-understanding and strategies that make meltdowns and shutdowns less frequent and less damaging when they do occur.
What Causes Autism Meltdowns and Shutdowns
Understanding what causes autism meltdowns vs shutdowns helps parents and autistic adults identify the triggers before the overload point is reached.
Both meltdowns and shutdowns are caused by the autistic nervous system reaching its capacity threshold. The specific triggers vary enormously between individuals but commonly include:
Sensory overload: Too much noise, too much light, an uncomfortable texture, an overwhelming smell, or any combination of sensory inputs that exceed the nervous system's regulatory capacity.
Demand overload: Too many demands placed too close together without adequate recovery time. This is particularly relevant for autistic individuals with a demand avoidance profile.
Emotional overload: Intense emotions, including positive ones like excitement, that exceed the nervous system's capacity to process and regulate.
Social overload: Extended social interaction that requires sustained masking, decoding of social cues, or management of unpredictable social dynamics.
Transition and change: Unexpected changes to routine or environment that remove the predictability the autistic nervous system depends on for regulation.
Cumulative load: This is one of the most important and most frequently missed causes. A meltdown or shutdown that appears to be triggered by something small is often the result of cumulative load building throughout the day or week, where the small thing was simply the last straw on top of an already overloaded system.
For autistic individuals who also have a demand avoidance profile, the specific interaction between demand overload and nervous system dysregulation is covered in detail in the post on pathological demand avoidance in autism.
The Warning Signs Before a Meltdown or Shutdown
Recognizing the warning signs before a meltdown or shutdown gives a window to intervene and reduce the load before the threshold is reached.
Early warning signs that apply to both:
Increased stimming beyond the person's baseline
Visible tension in the body including clenched hands, tight jaw, or hunched shoulders
Increased irritability or emotional reactivity to things that would not normally produce that response
Reduced verbal communication or shorter, less complex responses
Seeking sensory input or sensory avoidance more strongly than usual
Difficulty transitioning between activities
Signs that a meltdown specifically is building:
Voice becoming louder or higher pitched
Increasing physical agitation including pacing or fidgeting
Emotional responses escalating rapidly
Signs that a shutdown specifically is building:
Becoming progressively quieter and more withdrawn
Reduced eye contact and social engagement
Appearing to disengage from the environment gradually
Tracking these warning signs over time, keeping notes about what preceded specific meltdowns and shutdowns, is one of the most effective ways to identify the specific pattern for a specific individual and build prevention strategies around it.
What Not to Do During Autism Meltdowns vs Shutdowns
Understanding what not to do during autism meltdowns vs shutdowns is as important as knowing what to do, because well-intentioned responses frequently make both significantly worse.
Do not:
Raise your voice or increase the emotional intensity of the environment
Issue demands, consequences, or ultimatums during the episode
Try to reason with, explain to, or lecture the person during the episode
Add physical contact without clear consent, particularly during meltdowns
Interpret either state as deliberate or manipulative behavior
Shame the person during or after the episode
Try to talk through what happened immediately afterward before adequate recovery time has passed
All of these responses add to the sensory and emotional load rather than reducing it, extending and intensifying the episode rather than supporting recovery.
After the Meltdown or Shutdown: Recovery
The recovery period after autism meltdowns vs shutdowns is an important and often overlooked part of the experience.
Both meltdowns and shutdowns are physically and neurologically exhausting. The period immediately afterward requires genuine recovery time before the person is ready to reengage with normal demands. Attempting to resume normal expectations too quickly is one of the most common mistakes and frequently triggers a second episode.
After adequate recovery time, gentle, low-pressure reconnection is often helpful. A simple check-in that communicates safety and non-judgment without requiring explanation or analysis of what happened is usually the right approach. Detailed debriefing of the episode is only useful much later, when the person is fully regulated and has chosen to discuss it, and even then should be led by the autistic person rather than the parent or caregiver.
Dropped in a Maze by Sonia Chand addresses the emotional complexity of navigating these kinds of experiences, the meltdowns, the shutdowns, the misunderstandings, and the recovery, with the kind of honesty and practical wisdom that is rare in autism literature.

Preventing Autism Meltdowns and Shutdowns
While autism meltdowns vs shutdowns cannot be prevented entirely, their frequency and intensity can be significantly reduced through proactive strategies.
Prevention strategies include:
Building sensory-friendly environments at home and school that reduce the baseline sensory load
Maintaining predictable routines that reduce the cognitive and emotional demands of daily navigation
Building genuine recovery time into every day, not as a reward but as a necessity
Monitoring cumulative load and reducing demands proactively when the load is already high
Using visual schedules to reduce transition-related anxiety
Identifying individual triggers through careful tracking and building avoidance or mitigation strategies around them
Reducing masking demands wherever possible, because sustained masking significantly depletes the regulatory capacity that meltdowns and shutdowns draw from
The On the Spectrum podcast with Sonia Chand covers these prevention strategies and the broader experience of autistic regulation in honest, practical conversations that are genuinely useful for both parents and autistic adults.
FAQs
What is the difference between autism meltdowns vs shutdowns?
Meltdowns are outward fight or flight responses to neurological overload. Shutdowns are inward freeze responses to the same overload. Both are involuntary.
Are autism meltdowns the same as temper tantrums?
No. Tantrums are goal-directed behaviors. Meltdowns are involuntary neurological responses to overload that the autistic person is not controlling.
Can autistic adults have meltdowns and shutdowns?
Yes. Meltdowns and shutdowns are not limited to children. Many autistic adults experience both regularly throughout their lives.
How long do autism meltdowns and shutdowns last?
Duration varies significantly. Meltdowns typically last minutes to an hour. Shutdowns can last hours or longer depending on the individual and the degree of overload.
What triggers autism meltdowns vs shutdowns?
Both are triggered by the autistic nervous system reaching its overload threshold, through sensory, emotional, social, or demand-related input or a cumulative combination of all of these.
Should I try to talk to an autistic person during a meltdown or shutdown?
Minimal verbal communication is best during both. The nervous system cannot process complex social and verbal information during either state.
How can I help prevent autism meltdowns and shutdowns?
Reduce sensory load, maintain predictable routines, build genuine daily recovery time, reduce masking demands, and monitor cumulative load proactively.
Final Thoughts
Autism meltdowns vs shutdowns are not behaviors to be managed through consequences or discipline. They are neurological events that happen when an autistic nervous system has reached its limit, and they require a response that is calibrated to what is actually happening rather than what it looks like from the outside.
Getting that response right, for parents and for autistic adults themselves, is one of the most practically valuable things to understand about autism. It changes the dynamic from confrontation to support, from frustration to compassion, and from making things worse to genuinely helping the person you love return to regulation.
That understanding is worth everything.
References:
Autism Society. Autistic Meltdowns and Shutdowns: An Inclusive Guide for Healthcare Professionals [Internet]. 2025 Jun. Available from:https://autismsociety.org/wp-content/uploads/2025/07/AutismSociety_Autistic-Meltdowns-Shutdowns_2025-06V2F_Digital.pdf
Leicestershire Partnership NHS Trust. Understanding autistic meltdowns and shutdowns [Internet]. Last modified 2025 Apr 28. Available from:https://www.leicspart.nhs.uk/autism-space/health-and-lifestyle/meltdowns-and-shutdowns/
Misheva E. Why an autistic meltdown or shutdown is not a 'tantrum' [Internet]. OpenLearn, The Open University; 2025 Feb 28. Available from:https://www.open.edu/openlearn/health-sports-psychology/why-autistic-meltdown-or-shutdown-not-tantrum
Steward R, Knight J. 1800 Seconds on Autism [audio podcast episode]. BBC Radio. Available from:https://www.bbc.co.uk/programmes/p08b5qyn

How to Support an Autistic Partner in a Relationship
How to support an autistic partner in a relationship is a question that comes up in two very different ways. Sometimes it is asked by the neurotypical partner trying to bridge a gap they cannot quite name. And sometimes it is asked by the autistic partner themselves, trying to understand why connection feels so complicated even when the love is completely genuine.
How to support an autistic partner in a relationship is not really one question. It is several layered ones. How do we communicate in ways that work for both of us? How do we navigate sensory differences, social exhaustion, and the aftermath of a lifetime of masking? How do we build something real and sustainable when one or both partners are working with a neurology the relationship world was not designed for?
This post answers those questions honestly, with research where it exists and with the kind of practical, human clarity that most relationship advice never quite gets to when autism is involved.
Table of Contents
How to Support an Autistic Partner: Starting With Understanding
The Double Empathy Problem: Why Communication Breaks Down
Communication Strategies That Actually Work
Sensory Needs in an Intimate Relationship
Social Exhaustion and What It Means for Couples
Masking in Relationships and the Cost of Dropping It
Conflict and Repair in Autistic Relationships
How to Support an Autistic Partner Through Burnout
Intimacy and Connection in Autistic Relationships
When to Seek Support
Helpful Resources
FAQs
Final Thoughts
How to Support an Autistic Partner: Starting With Understanding
How to support an autistic partner in a relationship starts before any specific strategy or communication technique. It starts with genuinely understanding what autism means for that specific person in that specific relationship, not the clinical definition, not the stereotype, but the real, lived experience of your partner navigating a world that was not designed for their neurology.
Autism in relationships does not look one way. An autistic partner might be the most loyal, most attentive, most deeply committed person you have ever been with, and simultaneously struggle profoundly with reading social cues, managing sensory input during intimacy, or recovering from a difficult social event quickly enough to be emotionally present that same evening.
Both of those things are true at the same time. And holding both of them, without resolving them into a simpler story, is the starting point for how to support an autistic partner in a relationship genuinely rather than performatively.
The Double Empathy Problem: Why Communication Breaks Down
One of the most important research findings for understanding how to support an autistic partner in a relationship is the double empathy problem, a concept developed by autistic researcher Dr. Damian Milton.
For decades, the autism narrative assumed that autistic people lacked empathy and that this was the primary source of relationship difficulties. The double empathy problem turns this on its head.Research by Milton published in Disability and Society found that the communication difficulties between autistic and neurotypical people are bidirectional. Neurotypical people struggle to understand autistic communication just as much as autistic people struggle to understand neurotypical communication. The difference is that only one group has been pathologized for it.
In a relationship, this means that communication breakdown is not one partner's fault. It is the result of two different neurological operating systems trying to interface without a shared manual. The solution is not for the autistic partner to communicate more neurotypically. It is for both partners to develop a shared language that works for both of them.
Understanding the double empathy problem reframes how to support an autistic partner in a relationship entirely. It replaces the narrative of one partner needing to try harder with a more accurate and more equitable story of two people building a bridge from both sides.
Intimacy and Connection in Autistic Relationships
How to support an autistic partner in a relationship around intimacy requires dropping assumptions about what intimacy should look like and replacing them with genuine curiosity about what it looks like for your specific partner.
Autistic people often experience and express love, connection, and intimacy differently from neurotypical norms. They may show love through acts of service, through sharing their special interests, through problem-solving for their partner, or through consistent presence rather than through physical affection or verbal expressions of emotion.
Research on attachment in autism has found that autistic individuals form genuine and deep attachments to their partners, but that the expression of those attachments often does not match neurotypical expectations. Learning to recognize the specific ways your partner expresses love and connection, rather than measuring them against neurotypical standards, fundamentally changes the experience of the relationship for both of you.
For autistic adults working to understand their own patterns of connection and build relationships that work with their neurology rather than against it, coaching with Sonia offers exactly the kind of personalised, neurodivergent-affirming support that makes that work possible.
Book a socio-emotional coaching session with Sonia here and start building the relationship skills and self-understanding that change how connection actually feels.
What to Do When Your Child Reacts With Distress
Not every child responds to the autism disclosure with immediate acceptance or relief. Some children respond with grief, anger, denial, or intense distress. All of these responses are valid and none of them mean you did anything wrong.
When your child responds with distress:
Stay present and calm without rushing to fix the feeling
Validate the emotion without reinforcing a negative framing of autism
Avoid minimizing: it is not that bad is not helpful, but neither is catastrophizing alongside them
Give them time and space to process before continuing the conversation
Connect them with other autistic children or adults whose lived experience reflects what is possible
The distress is almost never really about the word autism. It is about the fear of what the word means for their future, their relationships, and how other people will see them. Addressing those fears directly and honestly, with genuine reassurance grounded in reality rather than false promises, is the most effective response.
Keeping the Conversation Going After the First Disclosure
How to tell your child they have autism is really a question about how to begin a lifelong conversation rather than how to have a single defining moment. The first disclosure is important, but what happens after it matters just as much.
Keep autism a normal part of family conversation. Reference it when it is relevant, not as a label that explains every difficulty but as a context that explains specific experiences. Allow your child to bring it up themselves. Answer their questions honestly as they evolve. Connect them with autistic community, books, media, and role models as they grow.
According to research. autistic individuals who grew up in families where autism was discussed openly and positively had significantly better autistic identity and mental health outcomes in adulthood than those for whom it was a topic that was avoided or discussed primarily in terms of challenges.
The conversation you start when you figure out how to tell your child they have autism is the first chapter of a much longer story. Make it a good one.
Dropped in a Maze by Sonia Chand is one of the most honest and practically grounded accounts of navigating the autism journey as a family, and it is exactly the kind of reading that helps parents find the words for conversations that feel impossibly hard before you start them.
Final Thoughts
How to tell your child they have autism is one of the most important conversations you will have as a parent. Not because it is the hardest, though it can feel that way, but because it is the beginning of your child's relationship with their own identity. The frame you use, the language you choose, and the ongoing conversation you commit to after the first disclosure all shape who your child believes themselves to be and what they believe is possible for them.
Get it right and you give your child the most powerful gift available: an accurate understanding of their own mind, offered with love, so they can spend their life building on who they actually are rather than apologizing for it.
References
Cooper K, Russell AJ, Lei J, Smith LGE. The impact of a positive autism identity and autistic community solidarity on social anxiety and mental health in autistic young people. Autism. 2023;27(3):848-857. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10074754/
Wheeler M. Getting Started: Introducing Your Child to His or Her Diagnosis of Autism [Internet]. Indiana Resource Center for Autism; 2020 May. Available from: https://iidc.indiana.edu/irca/resources/learn-about-autism/getting-started-introducing-your-child-to-his-or-her-diagnosis-of-autism.html

What Are the Management of Autism: Complete Guide
What are the management of autism is one of the most searched questions by parents who have just received a diagnosis and by autistic adults who are trying to build a life that actually works for their neurology. And it is a question that deserves a genuinely useful answer, not a list of clinical interventions that leaves you more overwhelmed than when you started.
What are the management of autism in the most accurate sense is not about fixing or curing autism. Autism is not something that needs to be fixed. It is a neurodevelopmental profile that requires the right understanding, the right environment, and the right support tools to allow the autistic person to genuinely thrive. The management of autism is therefore better understood as the set of strategies, therapies, accommodations, and approaches that help autistic individuals live well as their authentic selves rather than constantly fighting against their own neurology.
This post covers what the management of autism actually involves across every major domain of life, what the research supports, and what genuinely helps versus what sounds helpful but does not deliver.
Table of Contents
What Are the Management of Autism: Framing It Correctly
Communication Support as Core Management of Autism
Behavioral and Therapeutic Approaches
Sensory Management as Part of Autism Management
Educational Management of Autism
Mental Health Management in Autism
Medical Management of Autism Co-occurring Conditions
Management of Autism Through Routine and Structure
Management of Autism for Adults
What Does Not Work in the Management of Autism
FAQs
Final Thoughts
References
What Are the Management of Autism
What are the management of autism starts with getting the frame right, because the frame determines everything about what approaches are pursued and what outcomes are expected.
The management of autism is not about eliminating autistic traits. Stimming, special interests, sensory sensitivities, and direct communication styles are not problems to be erased. They are features of an autistic neurology that, in the right environment, are not just acceptable but genuinely valuable. The management of autism that produces the best long-term outcomes is always the management that works with the autistic neurology rather than against it.
What are the management of autism when framed correctly looks like this: strategies that reduce the barriers between autistic individuals and the life they deserve, accommodations that make environments more navigable for autistic brains, therapies that build genuine skills rather than performing neurotypicality, and support systems that reduce the anxiety and exhaustion that come from navigating a world not designed for autistic neurology.
With that frame in place, here is what effective management of autism actually involves.
Communication Support as Core Management of Autism
Communication support is one of the most consistently impactful forms of management of autism, particularly for children, and the research supporting it is among the strongest in the entire field.
For autistic children who are developing verbal language, speech and language therapy focused on functional communication, social use of language, and processing differences is a core component of effective management of autism. For children who are nonverbal or minimally verbal, Augmentative and Alternative Communication, known as AAC, is one of the most transformative interventions available.
Research published in the American Journal of Speech-Language Pathology consistently shows that early AAC introduction does not prevent spoken language development and in many cases actively supports it by providing a reliable communication channel during the critical developmental window.
The principle underlying communication as management of autism is simple: when a person can communicate their needs, preferences, and experiences reliably, almost every other area of functioning improves. Communication is not one part of the management of autism. It is the foundation everything else builds on.
Behavioral and Therapeutic Approaches
When parents ask what are the management of autism in terms of formal therapeutic intervention, behavioral and developmental approaches are usually what they are thinking of.
Applied Behaviour Analysis: ABA is the most extensively researched behavioral intervention in autism and it is also the most debated. Modern naturalistic ABA approaches that focus on skill development through child-led play and genuine functional goals have stronger evidence and broader endorsement than older discrete trial formats that focused primarily on compliance and suppression of autistic traits. A comprehensive review found that naturalistic developmental behavioral interventions showed positive outcomes across communication, social skills, and daily living skills.
DIR Floortime: The Developmental, Individual Difference, Relationship-based model uses child-led play and relationship as the vehicle for developmental progress. It is widely endorsed by autistic advocates as more affirming than purely behavioral approaches.
Occupational Therapy: OT addresses sensory processing, fine motor development, and daily living skills. It is one of the most consistently useful components of management of autism across age groups and support levels.
Cognitive Behavioral Therapy: CBT adapted for autism has a growing evidence base for addressing the anxiety and depression that frequently co-occur with autism, particularly in individuals with good verbal ability.
Sensory Management as Part of Autism Management
What are the management of autism without addressing sensory processing? Incomplete, because sensory differences affect nearly every autistic individual and significantly shape their capacity to function in different environments.
Effective sensory management as part of autism management includes:
Environmental modifications at home and school such as lighting adjustments, noise reduction, and sensory-friendly spaces
Sensory diets, structured schedules of sensory activities developed with an occupational therapist, that provide regulatory input throughout the day
Access to sensory tools including noise-cancelling headphones, weighted blankets, and fidget tools
Teaching sensory awareness so autistic individuals can identify their own sensory needs and communicate them
Sensory management is not about eliminating sensory sensitivities. It is about reducing unnecessary sensory load and providing appropriate sensory input so the nervous system can stay regulated enough to engage with learning, relationships, and daily life.
Educational Management of Autism
The educational management of autism is one of the most practically significant domains for families because school occupies so much of a child's daily life and has such a long-term influence on outcomes.
Effective educational management of autism includes an IEP that genuinely reflects the child's specific profile, communication needs, sensory requirements, and learning style. It includes trained educators who understand autism as a neurodevelopmental difference rather than a behavioral problem. It includes flexible assessment approaches that allow autistic students to demonstrate knowledge through channels that work for their brain. And it includes explicit social skills support and transition planning for older students.
What are the management of autism in school settings should always start from the legal entitlements of the autistic student. Under IDEA, every autistic child is entitled to a Free Appropriate Public Education with the support and services they need to benefit from it.
For parents who are navigating the school system and want a complete picture of what their child is legally entitled to and how to advocate for it effectively, the post on autism and the legal system rights and protections covers the full legal framework in detail.
Mental Health Management in Autism
What are the management of autism cannot be answered without addressing mental health, because the mental health burden of being autistic in a world designed for neurotypical brains is real, significant, and frequently underaddressed.
Anxiety affects between 40 and 60 percent of autistic individuals. Depression is also significantly more common in autistic people than in the neurotypical population. Autistic burnout, the collapse of functioning that results from sustained masking and demand overload, is a significant risk for autistic individuals of all ages and support levels.
Effective mental health management as part of autism management includes therapy adapted for autistic communication styles, reduction of masking demands through environmental accommodation, access to coaching that builds genuine self-understanding rather than performed neurotypicality, and connection with autistic community that reduces the social isolation that significantly worsens mental health.
Mental health management of autism is one of the areas where Sonia's coaching practice makes the most direct difference, working with autistic individuals and their families to build the self-understanding, emotional regulation strategies, and identity foundation that clinical therapy alone does not always reach.
Book a coaching session with Sonia here and get the mental health support that is built around your actual autistic neurology rather than a neurotypical template.
Medical Management of Autism Co-occurring Conditions
What are the management of autism also includes the medical management of the co-occurring conditions that affect a significant proportion of autistic individuals.
These include epilepsy, which affects approximately 30 percent of autistic individuals and requires specific anticonvulsant management, gastrointestinal disorders including constipation and gut motility issues that are common in autism and significantly affect behavior and wellbeing when unaddressed, sleep disorders that affect between 40 and 80 percent of autistic individuals and have downstream effects on every other area of functioning, and attention deficit hyperactivity disorder which co-occurs with autism in approximately 30 to 50 percent of cases and may require specific medication and behavioral management.
Medical management of these co-occurring conditions is an important and often overlooked component of comprehensive autism management. Addressing a gastrointestinal issue or a sleep disorder can produce significant improvements in behavior, regulation, and learning that no amount of behavioral intervention would have achieved, because the underlying physical cause was driving the difficulty.
Management of Autism Through Routine and Structure
One of the most accessible and most consistently effective components of management of autism is also one of the simplest: predictable routine and visual structure.
Autistic brains generally process predictable information more efficiently than unpredictable information, and the anxiety that drives many of the most challenging autism-related behaviors is significantly reduced when the environment is structured and transitions are anticipated.
Effective routine and structure as management of autism includes visual schedules that make the sequence of daily activities visible and accessible, transition warnings that give advance notice of upcoming changes, consistent daily routines that reduce the cognitive load of navigating daily life, and clear, explicit communication of expectations rather than reliance on implied or inferred social rules.
Management of Autism for Adults
What are the management of autism for adults is a question that receives far less attention than it deserves, because autism does not end at age 18 and the management needs of autistic adults are both real and frequently unaddressed.
Effective management of autism for adults includes workplace accommodations including written instructions, flexible scheduling, sensory-friendly environments, and clearly defined expectations. It includes access to adult autism services including supported employment, independent living support, and mental health services adapted for autistic communication styles. It includes self-advocacy skills that allow autistic adults to request and negotiate the accommodations they need.
It also includes the most underrated component of adult autism management: genuine self-understanding. Autistic adults who understand their own neurology accurately, who know what drains them and what regulates them, who can identify their sensory needs and their communication preferences, are significantly better equipped to build sustainable lives than those who are still trying to function as neurotypical people without the right tools.
Dropped in a Maze by Sonia Chand is the book that gives autistic individuals and their families exactly that kind of grounded, honest self-understanding. It is one of the most practical and humanly real accounts of navigating an autism journey without a map, and it is the reading that many adults and parents wish they had found much earlier.
Also, the On the Spectrum podcast with Sonia Chand covers the management of autism in all its real, practical complexity, with guests and conversations that go beyond theory into the honest, lived experience of what actually helps.
What Does Not Work in the Management of Autism
What are the management of autism also requires being honest about what does not work, because ineffective approaches in autism management are not just unhelpful, they can actively cause harm.
Approaches that focus on eliminating autistic traits rather than supporting autistic functioning are associated with higher rates of anxiety, depression, and autistic burnout. Approaches that use punishment or aversive consequences to change autistic behavior are not evidence-based and are harmful. Unproven biomedical interventions including chelation therapy, bleach treatments, and restrictive diets without documented medical need have no credible evidence base and carry real risks of harm.
The management of autism is most effective when it starts from the position that the autistic person is a whole human being whose neurology deserves to be understood and accommodated rather than corrected.
FAQs
What are the management of autism?
The management of autism includes communication support, behavioral and developmental therapy, sensory accommodation, educational support, mental health management, medical management of co-occurring conditions, and routine and structure.
Is there a cure for autism that the management of autism is working toward?
No. Autism is a neurodevelopmental profile, not a disease. The management of autism aims to support autistic individuals in living well as their authentic selves, not to eliminate autism.
What is the most effective management of autism for young children?
Early communication support, sensory integration therapy, and naturalistic developmental behavioral intervention during the critical early years produce the strongest outcomes.
Can adults benefit from the management of autism?
Yes. Management of autism is beneficial across the entire lifespan and includes workplace accommodations, mental health support, self-advocacy skill building, and community connection for adults.
Is medication part of the management of autism?
Medication is not used to treat autism itself but may be used to manage specific co-occurring conditions including anxiety, ADHD, epilepsy, and sleep disorders.
What is the most important thing in the management of autism?
Starting from a genuine understanding and acceptance of the autistic person's neurology and building support that works with that neurology rather than against it.
Final Thoughts
What are the management of autism is ultimately a question about what it takes to help an autistic person live well in a world that was not designed for their brain. The answer is not a single intervention or a simple protocol. It is a comprehensive, individualized, genuinely affirming approach that addresses communication, sensory needs, mental health, education, and the daily structures that make life navigable.
The management of autism that produces the best outcomes is always the management that sees the autistic person clearly, understands their specific neurology accurately, and builds support around who they actually are rather than who the system wishes they were.
References
Lorang E, Maltman N, Venker C, Eith A, Sterling A. Speech-Language Pathologists' Practices in Augmentative and Alternative Communication during Early Intervention. Augment Altern Commun. 2022;38(1):41-52. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9549491/
Avula S, Mandefro BT, Sundara SV, et al. The Impact of Early Intensive Behavioral and Developmental Interventions on Key Developmental Outcomes in Young Children With Autism Spectrum Disorder: A Narrative Review. Cureus. 2025;17(9):e92055. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12514992/
U.S. Department of Education, Office of Special Education Programs. About IDEA [Internet]. Available from: https://sites.ed.gov/idea/about-idea/
Shenoy M, Indla V, Reddy H. Comprehensive Management of Autism: Current Evidence. Indian J Psychol Med. 2017;39(6):727-731. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5733418/
Mayo Clinic Staff. Autism spectrum disorder - Diagnosis and treatment [Internet]. Mayo Clinic; 2025 May 22. Available from: https://www.mayoclinic.org/diseases-conditions/autism-spectrum-disorder/diagnosis-treatment/drc-20352934

Navigating IEPs and Parenting on the Spectrum
When a family goes through divorce, the stakes are high for any child. When that child is autistic, the stakes become something else entirely. The decisions made in a courtroom, or ideally kept out of one, about education, therapy, medication, and daily routine can shape an autistic child's entire developmental trajectory.
Christopher Anderson knows this from two directions. He is a family law attorney licensed in Georgia, New York, and Colorado, where he runs a family law firm that specializes in helping families navigate divorce and co-parenting disputes. He is also the father of an 18-year-old with autism spectrum disorder, diagnosed at age three, who he has spent fifteen years advocating for through school systems, healthcare providers, and every other institution that needed reminding that his son was a human being first and a diagnosis second.
Christopher joined Sonia on the On the Spectrum podcast for one of the most practically useful conversations the show has hosted, covering what parents need to know about keeping the court out of parenting decisions, how to advocate effectively in IEP meetings, and what to do when the system tells you there is no budget for what your child needs.
If you want to hear the full conversation in Christopher's own words, listen to the full episode of On the Spectrum with Sonia here.
Table of Contents
Why Divorce Rates Rise When Special Needs Are Involved
The Core Philosophy: Keep the Decision With the Parents
What Best Interest of the Child Actually Means Legally
The Gandhi Story That Explains Everything
What Christopher Learned Advocating for His Own Son
When the School Says There Is No Budget
What to Do When the IEP Does Not Include What Your Child Needs
How to Advocate When You Do Not Have Money or Power
The Label Problem and Why It Matters
Where to Find Christopher Anderson
Final Thoughts
Why Divorce Rates Rise When Special Needs Are Involved
Research has consistently shown that divorce rates are higher in families raising children with special needs, and Christopher addressed this directly in the episode with a clarity that most legal professionals do not bring to the conversation.
The reason, he explained, is not simply stress. It is the collision of fundamentally different belief structures about the child and their needs. On one end of the spectrum, you have the parent who sees only the special needs and becomes overprotective, wanting to shield the child from every challenge the world might present. On the other end, you have the parent who wants to deny that there are any special needs at all.
When those two positions meet in a divorce proceeding, the conflict is not just emotional. It is expensive. Courts need to be educated about what is in the best interest of the child, and that education requires experts, developmental scientists, educational psychologists, and the kind of protracted litigation that drains families financially and emotionally over years.
Christopher's firm exists, in large part, to prevent that from happening.
The Core Philosophy: Keep the Decision With the Parents
The most important thing Christopher said in the entire episode is worth stating clearly: turning parenting decisions over to a court is a failure of empowerment.
His firm's motto is that they empower families to make the best decisions for themselves and for their children. In the context of autism and special needs, this means working relentlessly to help parents find common ground before a judge has to substitute their judgment for the parents'.
Courts can make decisions. But courts do not know your child. They do not know how your child wakes up in the morning, what sounds overwhelm them, what environments help them regulate, or what their genuine strengths look like under the right conditions. The parents know those things. Keeping that knowledge in the room where decisions are made, rather than handing it to a legal process that operates in generalities, is always the better outcome.
Christopher put it simply: his favorite words are that mommy and daddy, or whatever combination of parents is involved, have decided together that this is in your best interest. Those words, spoken to a child, carry a different weight than a court order.
What Best Interest of the Child Actually Means Legally
Best interest of the child is the legal standard in Colorado, Georgia, New York, and most states across the country when courts are making decisions about children in family law proceedings. But as Christopher explained, it is not a black and white standard.
Unlike a damages calculation or a negligence finding, best interest is a subjective analysis. The court is weighing evidence and opinion from multiple sources, including expert witnesses, developmental specialists, educators, and mental health professionals, to arrive at a conclusion that is necessarily shaped by the specific judge, the specific evidence presented, and the specific circumstances of the family.
This is why Christopher urges parents to do the work of gathering that expert information themselves, together, before the court ever needs to weigh in. If both parents bring a developmental specialist's report to the table, read it together, and engage with it genuinely, there is a real chance that the information itself closes the gap between their positions. The expert's conclusion about what the child needs can do the work that arguments between parents cannot.
If you are navigating a co-parenting dispute that involves your autistic child's education and legal rights, the post on autism and the legal system rights and protections covers the federal legal framework that applies to your child's educational entitlements and is worth reading before any IEP or court-related meeting.
The Gandhi Story That Explains Everything
Christopher shared a story in the episode that is worth repeating here in full, because it captures the spirit of everything he does as both a lawyer and a parent.
A mother brings her young child to Gandhi, having waited in line for hours, and asks him to tell her son to stop eating sugar. Gandhi tells her to come back in a month. She is frustrated but complies. A month later, she returns. Gandhi looks at the boy and says: stop eating sugar. The mother is furious. You could have said that a month ago. Gandhi replies: a month ago, I was eating sugar.
Christopher applies this story to his own credibility as an advisor. It is easy, he said, to tell parents to set aside their emotions and focus on what is best for their child. It is another thing entirely to have actually done that for fifteen years, through a divorce, through IEP battles, through every institutional encounter that required him to fight for his son while remaining focused on the outcome rather than the frustration.
He comes to that advice, he said, with some level of integrity. And it is not easy. But it is worth it.
The navigation of that journey, the emotional complexity of advocating for a child you love in systems that do not always make it easy, is something that Dropped in a Maze by Sonia Chand speaks to directly. It is the book that gives families the map that nobody hands you when the diagnosis arrives, and it is one of the most honest accounts of what this journey actually looks like from the inside.
What Christopher Learned Advocating for His Own Son
Christopher's son is now 18 and, by his father's account, has had a successful launch into adulthood. That outcome did not happen by accident. It happened because Christopher spent fifteen years applying the same philosophy at school IEP meetings that he applies in his legal practice: this is a human being, not a diagnosis, and the goal is his successful launch into life, not the smooth running of your system.
His biggest challenge, he said, was the institutional desire to medicate. Not because medication is wrong, but because the system's motivation for recommending it was often to make the system run more smoothly rather than to make the child thrive more fully. Across his blended family, which includes children with ADHD alongside his son with autism, he encountered this pattern repeatedly.
His response was always the same. Meet this child where they are. The label can help you understand certain behaviors better than you would without it. But it does not tell you much more than that. Do not think you know my child because you know his diagnosis.
That insistence on seeing the individual behind the diagnosis is not just good parenting advice. It is good clinical advice, good educational advice, and, Christopher argues, the foundation of any effective advocacy.
When the School Says There Is No Budget
Every parent of an autistic child has heard it. We do not have the budget for that. Christopher addressed this directly and practically in the episode.
His first point is one that reframes the entire conversation: budgets are about priorities. When a school says there is no budget, what they are really saying is that the money has been allocated to other priorities. That is a policy choice, not an immutable fact, and it can be challenged.
Here is what Christopher recommends when you hit the budget wall:
Take the request up the chain. If the IEP team refuses, go to the principal. If the principal refuses, go to the superintendent. Keep going.
Recognize that you are a burr in the system's desire to run smoothly, and use that strategically. Systems often bend to persistent, organized, documented advocacy.
Get involved at the school board level. Budget decisions are made there, and parent voices at school board meetings matter.
Join advocacy groups who can add their voice to yours, write letters, attend meetings, and connect you with organizations that provide grants to schools.
If you have the ability, consider whether moving to a better-resourced school district is an option, as Christopher himself did when his son was young.
What to Do When the IEP Does Not Include What Your Child Needs
Christopher's practical advice on IEPs was specific and actionable. When a pediatrician's recommendation, a therapist's recommendation, or an occupational therapist's recommendation is not being included in the IEP, the approach is straightforward.
Bring the paperwork. Put every professional recommendation on the table in writing. If the school refuses to include it in the IEP, escalate. Principal, superintendent, district level, and if necessary, legal advocacy. There are lawyers who specialize specifically in representing parents before schools in IEP disputes, and Christopher spoke highly of the ones who genuinely represent families rather than simply the district.
He also made a point that is worth highlighting for every parent navigating the IEP process: IEPs are reviewed once a year, but children grow and change throughout the year. Advocating for flexibility within the IEP, for the ability to revisit and adjust as the child's needs evolve, is just as important as advocating for the right provisions at the annual review.
Coaching with Sonia offers exactly the kind of personalised support that helps parents walk into IEP meetings prepared, confident, and clear about what they are entitled to ask for and how to ask for it effectively.
Book a coaching session with Sonia here and get the support that helps you advocate from a place of clarity rather than overwhelm.
How to Advocate When You Do Not Have Money or Power
One of the most important moments in the episode came when Sonia pushed back on the assumption that advocacy requires resources. What about the single mother who is struggling to make ends meet and has a special needs child on top of that?
Christopher's response was direct: advocacy is not primarily about money. It is about voice. And if your voice alone is not enough, join it with others.
Advocacy groups for special needs children exist everywhere and they can add organizational weight, legal knowledge, and community connections to what a single parent cannot accomplish alone. They can write letters to superintendents. They can attend IEP meetings. They can connect families with grant-providing organizations. They can direct you to state and federal representatives who need to hear from constituents about where educational funding should be going.
The political dimension of advocacy matters too. School board seats, state legislative offices, and federal representatives all make decisions that affect what resources are available to autistic children. Adding your voice to those conversations, individually and collectively, is part of the advocacy landscape that extends beyond the individual IEP meeting.
The Label Problem and Why It Matters
Christopher returned several times throughout the conversation to what he called the label problem, the tendency of schools, healthcare providers, and other institutions to think they understand a child once they have a diagnosis.
Oh, he has autism spectrum disorder. I know him now.
You know nothing, Christopher said. The label can help you understand certain behaviors in context. That is all it does. It does not tell you who this child is, what they love, what environments help them thrive, or what their genuine potential looks like with the right support around them.
This insistence on the individual over the label is the thread that runs through everything Christopher shared in this episode, from his legal philosophy to his parenting to his school advocacy. Every child with autism is still, first and foremost, a child. And the job of every adult in that child's life, whether parent, lawyer, teacher, or therapist, is to see the child clearly enough to serve them well.
The On the Spectrum podcast with Sonia Chand exists precisely for these kinds of conversations, the ones that go beyond the clinical and into the real, human complexity of raising, supporting, and advocating for autistic children in a world that does not always make it easy.
Where to Find Christopher Anderson
Christopher Anderson and his family law firm can be found atwww.newleaf.family. He is also active on LinkedIn and across social media platforms. His firm specializes in empowering families through divorce and co-parenting disputes, with particular experience supporting families with special needs children.
Final Thoughts
Christopher Anderson spent fifteen years learning, in real time, what it means to advocate for an autistic child through every institution that needed to be reminded that the child was a person first. He built a legal practice around the same principle. And he came to the On the Spectrum podcast to share what he has learned with the families who need it most.
The core message is simple even when the implementation is hard: keep the decision with the parents. Know your legal rights. Make the pie bigger. See your child as an individual, not a label. And when the system pushes back, which it will, push back harder, smarter, and with more voices alongside yours.
Your child's successful launch, as Christopher calls it, is the goal. Everything else is in service of that.
References:
Chand SK, Christensen V. Blueprints for Empowerment: Navigating IEPs and Parenting on the Spectrum with Vicki Christensen [audio podcast episode]. In: On the Spectrum Empowerment Stories with Sonia Krishna Chand. 2026 Jul 8. Available from:https://www.buzzsprout.com/2307116/episodes/19463789-blueprints-for-empowerment-navigating-ieps-and-parenting-on-the-spectrum-with-vicki-christensen
American Speech-Language-Hearing Association. Individualized Education Programs (IEPs), Individualized Family Service Plans (IFSPs), and Section 504 Plans [Internet]. Available from:https://www.asha.org/slp/schools/ieps/
National Council of Juvenile and Family Court Judges. A Judicial Guide to Child Safety in Custody Cases [Internet]. Available from:https://www.ncjfcj.org/bench-cards/a-judicial-guide-to-child-safety-in-custody-cases/
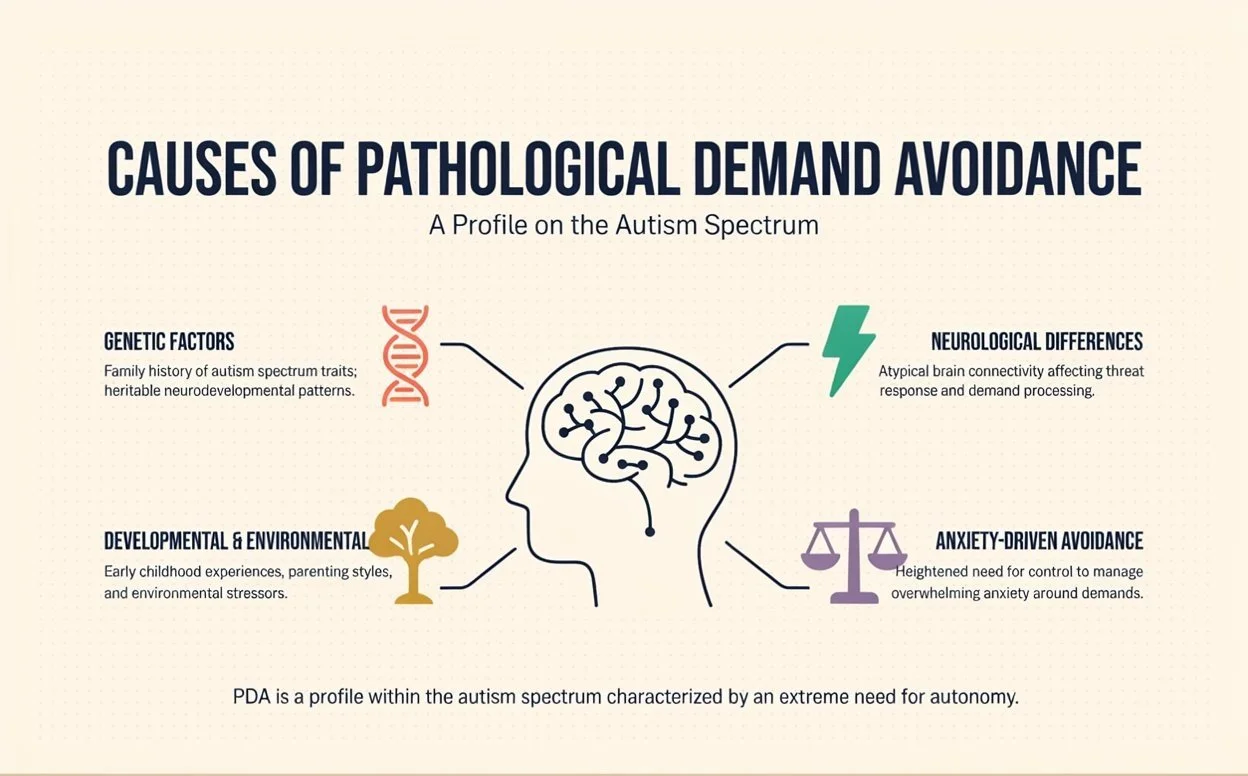
Causes of Pathological Demand Avoidance
The causes of pathological demand avoidance is one of the most searched and least clearly answered questions for parents and adults who have encountered this profile and are trying to understand where it comes from. If you are looking for a straightforward explanation of the causes of pathological demand avoidance that goes beyond vague references to anxiety and genetics, this post gives you exactly that.
Understanding the causes of pathological demand avoidance matters because the explanation shapes the response. When you understand what is actually driving the profile neurologically and developmentally, the interventions that help and the ones that make things significantly worse both start to make much more sense.
This post covers what the research currently says about the causes of pathological demand avoidance, what we know with confidence, what is still being investigated, and what it all means practically for the people living with this profile and the families supporting them.
Table of Contents
What Is Pathological Demand Avoidance?
The Causes of Pathological Demand Avoidance: Where the Research Points
Neurological Causes of Pathological Demand Avoidance
Genetic Causes of Pathological Demand Avoidance
The Role of Anxiety in Pathological Demand Avoidance
What Understanding the Causes Changes About Support
Is Pathological Demand Avoidance Caused by Parenting
Causes of Pathological Demand Avoidance vs Other Autism Profiles
What Does Not Cause Pathological Demand Avoidance
Final Thoughts
References
What Is Pathological Demand Avoidance?
Before going into the causes of pathological demand avoidance specifically, a brief overview of the profile itself helps frame what the causes need to explain.
Pathological demand avoidance is a profile within the autism spectrum, first identified by British psychologist Elizabeth Newson in the 1980s, characterized by an extreme and pervasive drive to avoid everyday demands and expectations. This avoidance is driven by anxiety about loss of autonomy and control rather than by defiance, laziness, or deliberate non-compliance.
People with pathological demand avoidance experience ordinary requests as genuine threats to their sense of safety. Their nervous system responds with a fight, flight, or freeze response to demands that most people process neutrally, and from that activated state, compliance becomes neurologically very difficult rather than simply undesirable.
For a full picture of what pathological demand avoidance looks like in daily life and how it differs from other autism profiles, the post on pathological demand avoidance in autism covers the profile comprehensively.
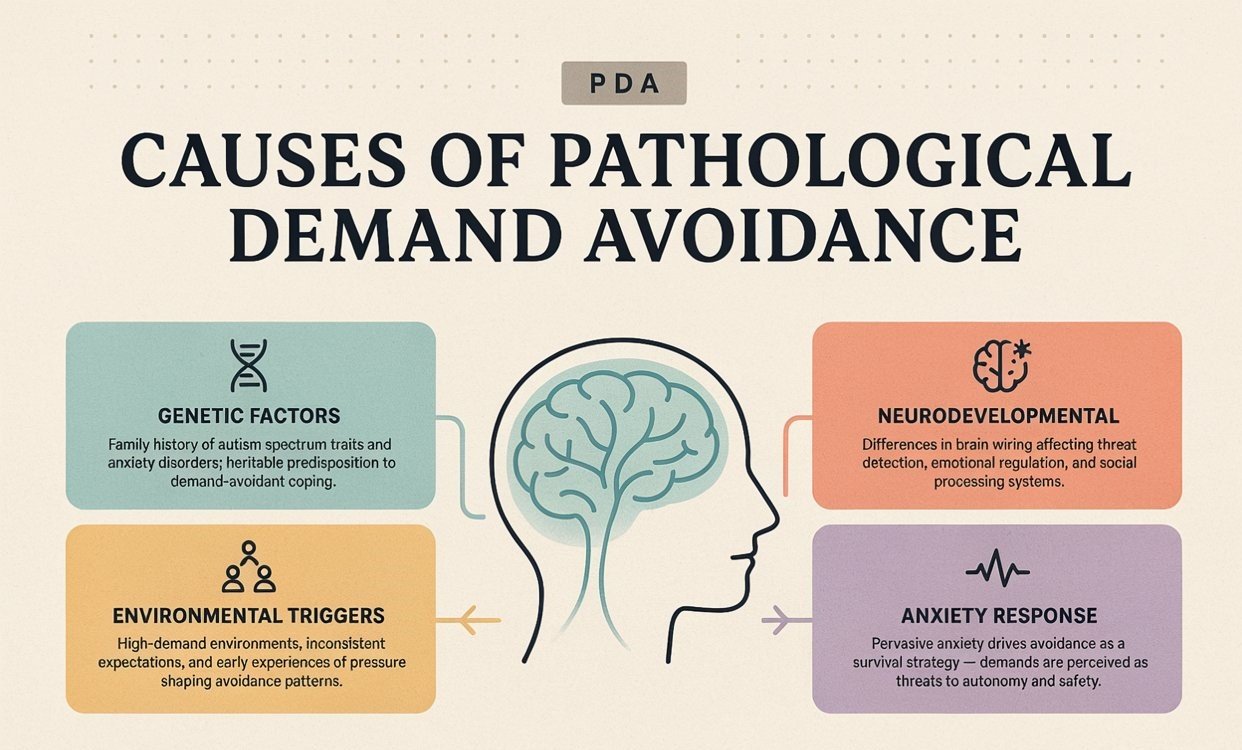
Causes of Pathological Demand Avoidance
The Causes of Pathological Demand Avoidance: Where the Research Points
The causes of pathological demand avoidance are currently understood to be neurological and genetic in origin, rooted in differences in brain development and nervous system functioning that are present from birth. This is important to state clearly at the outset because one of the most harmful misconceptions about pathological demand avoidance is that it is caused by parenting, trauma, or a child's deliberate choice.
It is none of those things.
The causes of pathological demand avoidance sit in the neurology and genetics of the individual, interacting with their environment in ways that either support or worsen the expression of the profile. Understanding this correctly from the beginning changes how everyone around the PDA individual responds to them.
Neurological Causes of Pathological Demand Avoidance
The neurological causes of pathological demand avoidance center on differences in how the brain processes threat, autonomy, and demand.
Research on pathological demand avoidance points toward differences in the functioning of the autonomic nervous system, particularly in how the threat detection system activates and regulates in response to perceived loss of control. In most people, a request or instruction is processed by the brain as neutral or mildly relevant information. In a person with pathological demand avoidance, the same request appears to activate the threat detection system, specifically the amygdala, in a way that generates a genuine anxiety and survival response.
Research by O'Nions and colleagues, published in the Journal of Child Psychology and Psychiatry found that children with PDA profiles showed distinct patterns of emotional and behavioral response to demands compared to other autistic children and to neurotypical children, supporting the idea that the neurological response to demands in PDA is genuinely different from typical processing.
The polyvagal theory, developed by Stephen Porges, offers a useful neurological framework for understanding one of the causes of pathological demand avoidance. The theory describes how the autonomic nervous system has three states: the ventral vagal state associated with safety and social engagement, the sympathetic state associated with fight or flight, and the dorsal vagal state associated with shutdown and freeze. In pathological demand avoidance, demands appear to reliably shift the nervous system out of the ventral vagal state and into sympathetic or dorsal vagal states, making genuine engagement and compliance neurologically very difficult.
This neurological explanation for one of the causes of pathological demand avoidance is also why standard behavioral approaches that work with neurotypical or even other autistic children are so consistently ineffective with the PDA profile. They attempt to use consequence and reward to change behavior that is driven by a nervous system threat response, which is the wrong level of intervention entirely.
Genetic Causes of Pathological Demand Avoidance
The genetic causes of pathological demand avoidance are not yet as well-mapped as the neurological ones, but the available evidence consistently points toward a strong heritable component.
Pathological demand avoidance clusters in families. Parents and siblings of children with PDA profiles frequently show PDA traits themselves, often undiagnosed, which is consistent with a genetic component to the causes of pathological demand avoidance.
Because pathological demand avoidance sits within the autism spectrum, its genetic causes are likely to overlap significantly with the genetics of autism more broadly. Autism is one of the most heritable neurodevelopmental conditions known to science, with genetic factors accounting for approximately 80 percent of autism risk. The specific genetic variants that contribute to a PDA presentation within the autism spectrum are still being investigated.
Research by Green and colleagues at the University of Manchester has begun to map the specific characteristics of the PDA profile more precisely, which is a necessary step toward identifying the specific genetic contributions to the causes of pathological demand avoidance separately from the broader genetics of autism.
What the current genetic evidence supports is that the causes of pathological demand avoidance are biological in origin, present from birth, and not the result of anything the family or individual has done or failed to do.
The Role of Anxiety in Pathological Demand Avoidance
Anxiety is not simply one of the consequences of pathological demand avoidance. It is arguably the central neurological mechanism through which the causes of pathological demand avoidance express themselves behaviorally.
The anxiety in pathological demand avoidance is specific. It is not generalized anxiety about many things. It is anxiety specifically triggered by the experience of demands and perceived loss of autonomy. This specificity is one of the reasons that standard anxiety interventions are often partially effective at best, because they address generalized anxiety without specifically addressing the autonomy-related trigger that drives pathological demand avoidance.
The anxiety response in pathological demand avoidance activates the same neurological pathways as any other threat response, releasing stress hormones, activating the amygdala, and shifting the nervous system into a defensive state. From that state, the cognitive resources needed for compliance, reasoning, and flexible response are significantly reduced. This is why PDA profiles respond to increased pressure with increased avoidance rather than increased compliance, which is the opposite of what most standard behavioral interventions predict.
Understanding anxiety as central to the causes of pathological demand avoidance is what makes the low-demand, high-autonomy approach the only genuinely effective framework for support. For a detailed breakdown of how that framework translates into specific language and strategies, the post on pathological demand avoidance language to use covers the practical application in full.
What Understanding the Causes Changes About Support
Understanding the causes of pathological demand avoidance changes everything about the support approach, and this is the most practically important part of this entire post.
When the causes of pathological demand avoidance are understood as neurological and anxiety-driven rather than behavioral and willful, the entire support framework shifts. Consequences and rewards become less relevant because they operate at the behavioral level without addressing the neurological driver. Pressure and structure become counterproductive because they increase the anxiety that is causing the avoidance. Autonomy and low demand become the most effective tools because they reduce the neurological threat response that makes compliance impossible.
This shift in understanding is genuinely difficult to make when you have been trained to think about behavior in behavioral terms, and it often requires skilled, informed support to put into practice consistently. Coaching with Sonia offers exactly that kind of personalised, neurodivergent-informed guidance for families working to translate their understanding of the causes of pathological demand avoidance into practical approaches that actually work day to day.
Book a coaching session with Sonia here and get the personalized support that helps you move from understanding the causes to actually building what helps.
Is Pathological Demand Avoidance Caused by Parenting
Is parenting one of the causes of pathological demand avoidance? This is one of the most important questions to answer clearly, because parents of PDA children are frequently blamed, implicitly or explicitly, for their child's behavior by professionals and family members who do not understand the profile.
Parenting is not one of the causes of pathological demand avoidance. Pathological demand avoidance is a neurological and genetic profile that is present from birth. It is not caused by inconsistent parenting, over-permissive parenting, over-controlling parenting, or any other parenting style.
What parenting can affect is how the environment around the PDA individual either supports or worsens the expression of the profile. Low-demand, high-autonomy parenting approaches reduce the anxiety driving pathological demand avoidance and create better conditions for engagement and functioning. High-demand, high-control parenting approaches increase the anxiety and worsen the avoidance. But neither creates the underlying neurological profile in the first place.
This distinction matters enormously for the mental health and self-perception of parents who have spent years being told, directly or indirectly, that they caused or are causing their child's pathological demand avoidance. They did not. And the support they need is not criticism or behavior management training. It is genuine understanding of what is actually happening neurologically and the practical tools to work with it.
Dropped in a Maze by Sonia Chand speaks directly to the experience of navigating a neurodivergent journey in a system that frequently misunderstands what it is seeing, and it offers the kind of honest, grounded perspective that helps parents stop questioning themselves and start understanding their child more accurately.
Causes of Pathological Demand Avoidance vs Other Autism Profiles
Understanding the causes of pathological demand avoidance in relation to other autism profiles helps clarify why PDA is considered a distinct profile within the spectrum rather than simply a more severe presentation of standard autism.
The core autism profile involves social communication differences, sensory processing differences, and restricted or repetitive behaviors. These features are also present in pathological demand avoidance, but in PDA the extreme anxiety-driven avoidance of demands is the most prominent and most functionally impairing feature, more so than in other autism profiles.
Research suggests that the causes of pathological demand avoidance may involve specific neurological differences in threat detection and autonomic regulation that are distinct from, or at least differently proportioned than, the neurological differences underlying other autism profiles. This would explain why PDA responds so differently to standard autism interventions, because the neurological driver of the most impairing features is different.
What Does Not Cause Pathological Demand Avoidance
Being equally clear about what does not cause pathological demand avoidance is as important as understanding what does.
The causes of pathological demand avoidance do not include:
Inconsistent or poor parenting
Trauma or adverse childhood experiences
Too much screen time or technology use
Dietary factors
Vaccines
Deliberate choices by the child or adult
Being spoiled or having boundaries set too loosely
Any form of environmental exposure
These are all factors that have been incorrectly attributed as causes of pathological demand avoidance by people who do not understand the neurological and genetic basis of the profile. None of them are supported by the research, and all of them lead to interventions that do not address what is actually happening and frequently make things worse.
Final Thoughts
The causes of pathological demand avoidance are neurological and genetic, rooted in genuine differences in how the brain responds to demands and perceived loss of control. They are not caused by parenting, by choice, or by any environmental factor within a family's control.
Understanding the causes of pathological demand avoidance accurately is the foundation of everything that follows, because what you believe is causing the behavior determines what you try to do about it. And the gap between effective and ineffective support for pathological demand avoidance is wide enough that getting the causes right genuinely changes lives.
References
PDA Society. Origins of term PDA [Internet]. 2025 Apr 11. Available from:https://www.pdasociety.org.uk/research-professional-practice/origins-of-term-pda/
Malik O, Baird G. Commentary: Conceptualising demand avoidance in an ASD context – a response to Osman Malik & Gillian Baird (2018). Child Adolesc Ment Health. 2018;23(4):387-388. Available from:https://pubmed.ncbi.nlm.nih.gov/32677136/
Nawaz S, Speer S. What are the experiences and support needs of families of autistic children with Extreme (or 'Pathological') Demand Avoidance (E/PDA) behaviours? Res Autism Spectr Disord. 2025;119:102515. Available from:https://www.sciencedirect.com/science/article/pii/S1750946724001909
O'Nions E, Gould J, Christie P, Gillberg C, Viding E, Happé F. Identifying features of 'pathological demand avoidance' using the Diagnostic Interview for Social and Communication Disorders (DISCO). Eur Child Adolesc Psychiatry. 2015;25:407-419. Available from:https://pmc.ncbi.nlm.nih.gov/articles/PMC4820467/
PDA Society. Research overviews [Internet]. Available from:https://www.pdasociety.org.uk/research-professional-practice/research-overviews/

What Is a Visual Schedule in Autism? A Complete Guide
A visual schedule for autism is one of the most practical, most researched, and most consistently effective tools available for supporting autistic children and adults across home and school settings. If you have been hearing about visual schedules for autism and wondering whether they actually work, how to make one, and whether your child or student genuinely needs one, this post answers all of those questions directly and honestly.
A visual schedule for autism uses images, symbols, photographs, or written words to represent the sequence of activities or tasks in a day or within a specific activity. Rather than relying on verbal instructions that may be difficult to process, retain, or act on, a visual schedule for autism gives the autistic person a concrete, predictable, and independently accessible representation of what is coming next.
This post covers the theory behind why visual schedules for autism work, the research supporting their use, how to build and implement one effectively, and what to do when they are not working as well as you hoped.
Table of Contents
What Is a Visual Schedule for Autism and Why Does It Work
Who Benefits Most From a Visual Schedule for Autism
Types of Visual Schedules for Autism
Visual Schedules for Autism at Different Ages
How to Build a Visual Schedule for Autism at Home
How to Implement a Visual Schedule for Autism at School
Visual Schedules for Autism and Transitions
Common Mistakes With Visual Schedules for Autism
When a Visual Schedule for Autism Is Not Enough
Final Thoughts
What Is a Visual Schedule for Autism and Why Does It Work
A visual schedule for autism works because it addresses several of the core processing differences that characterize autistic neurology simultaneously.
Autistic individuals frequently experience challenges with working memory, which is the ability to hold and manipulate information in the mind over short periods. Verbal instructions, which require the listener to hear, process, retain, and act on spoken information, place significant demands on working memory. For many autistic children and adults, verbal instructions simply do not stay accessible long enough to act on them reliably.
A visual schedule for autism removes the working memory demand by making the information permanently visible and accessible. The autistic person does not need to remember what comes next. They can look at the schedule and see it.
Visual schedules for autism also address the deep autistic need for predictability and routine. Unexpected changes are one of the most consistently distressing experiences for autistic individuals across the spectrum. A visual schedule for autism creates a concrete, visible representation of what the day holds, reducing the uncertainty that drives much of the anxiety and distress that autistic children and adults experience around transitions and unexpected events.
Finally, visual schedules for autism support independence. Rather than needing to ask a teacher or parent what comes next, an autistic child with access to a well-designed visual schedule can navigate transitions and activities with significantly more autonomy, which is both practically beneficial and deeply affirming for a population that often has very little control over their environment.
Who Benefits Most From a Visual Schedule for Autism
Visual schedules for autism are beneficial across the spectrum, but some autistic individuals benefit more immediately and more dramatically than others.
Children and adults who benefit most from a visual schedule for autism include those who:
Struggle significantly with transitions between activities
Experience high anxiety around unexpected changes to routine
Have difficulty following multi-step verbal instructions
Show significant distress at the end of preferred activities
Are working on building independence in daily routines
Have limited or no functional spoken language and rely on visual processing
Visual schedules for autism are not only for young children or for those with significant support needs. Many autistic teenagers and adults use visual schedules and visual planning tools because they genuinely support executive functioning in ways that no amount of effort or willpower can replicate without them.
Types of Visual Schedules for Autism
Visual schedules for autism come in several different formats, and choosing the right one for your specific child or student matters significantly.
Object schedules: For very young children or those with significant support needs, real objects representing each activity can be used. A cup for snack time, a book for reading, a shoe for outdoor time. Object schedules are the most concrete level of visual representation and work well for children who are not yet reliably processing photographs or symbols.
Photograph schedules: Photographs of the actual activities, environments, and materials involved in each part of the day. Photographs are highly concrete and immediately recognizable, making them effective for children who are beginning to process visual representations.
Symbol or picture communication schedules: Standardized symbol systems such as PCS symbols from Boardmaker or Widgit symbols provide a consistent visual language that can be used across home and school settings. These work well for children who have moved beyond needing photographs to recognize activities.
Written schedules: For autistic individuals with functional reading skills, written schedules provide all the same benefits as picture-based schedules with the added efficiency of text.
Digital schedules: Apps and digital tools that provide visual scheduling on tablets or phones are increasingly popular and offer the significant advantage of always being accessible to the individual wherever they are.
Building a Visual Schedule for Autism at Home
How to Build a Visual Schedule for Autism at Home
Building an effective visual schedule for autism at home does not require specialist materials or significant expense. Here is a practical framework:
Step one: Identify the routine you are scheduling
Start with one specific routine rather than the entire day. Morning routines, bedtime routines, and homework sequences are common starting points. A focused visual schedule for autism is more effective than an overwhelming whole-day representation for many children.
Step two: List every step in the routine
Write down every individual step in the routine in sequence. Be more specific than you think you need to be. Get dressed is not one step. It is underwear, then socks, then trousers, then shirt, then shoes.
Step three: Choose the right visual format
Match the visual format to your child's current level of visual processing. Start concrete with photographs or objects if unsure, and move toward symbols or text as understanding develops.
Step four: Present the schedule at the start of the routine
Go through the visual schedule for autism with your child before the routine begins, pointing to each step in sequence. This primes the brain for what is coming rather than introducing each step as a surprise.
Step five: Allow the child to interact with the schedule
Where possible, allow the child to move or check off completed items on the visual schedule for autism. This interaction with the schedule increases engagement and reinforces the connection between the visual representation and the actual activity.
Navigating the practicalities of implementing tools like visual schedules for autism at home, alongside all the other demands of raising an autistic child, is genuinely challenging and the learning curve is real. Dropped in a Maze by Sonia Chand is the book that so many parents wish had existed when they were starting out, an honest, practical account of navigating the autism journey without a map.
Visual Schedules for Autism at Different Ages
Visual schedules for autism are not only for young children and their benefits extend across the lifespan.
For toddlers and preschoolers, object and photograph schedules support the development of routine understanding and transition compliance during the most developmentally sensitive period for establishing predictable structure.
For school-age children, visual schedules support academic task completion, homework routines, and the increasingly complex social and academic schedule of the school day.
For teenagers, visual scheduling tools support executive functioning, homework management, and the self-directed organization that secondary school increasingly demands.
For autistic adults, visual planning tools including apps, written schedules, and structured daily planners serve the same fundamental function, reducing the cognitive load of executive functioning and making the day more predictable and more manageable.
If you are an autistic adult who has discovered that visual scheduling tools genuinely help you, or a parent supporting an autistic teenager who is developing their own organizational strategies, coaching with Sonia offers personalised support for building the practical life management tools that work with your specific neurology rather than against it.
Book a coaching session with Sonia here and get personalised support for building the daily structure that actually works for your brain.
How to Implement a Visual Schedule for Autism at School
Implementing a visual schedule for autism in a school setting involves several additional considerations beyond the home implementation framework.
Consistency across adults: Every adult who works with the child needs to use the visual schedule for autism in the same way. Inconsistency in how the schedule is presented or referenced significantly reduces its effectiveness.
Placement: The visual schedule for autism needs to be placed where the child can independently access and reference it throughout the day. A schedule that lives on the teacher's desk is not independently accessible and defeats one of the primary purposes of the tool.
Previewing transitions: Before each transition, direct the child's attention to the visual schedule for autism to preview what is coming next. This brief preview significantly reduces transition-related distress because the change is no longer unexpected.
Incorporating the child's input: Where possible, involve the autistic child in building and maintaining their visual schedule for autism. Children who have some ownership of their schedule engage with it more reliably than those for whom it is simply imposed.
Including preferred activities: A visual schedule for autism that includes only demands and transitions and no preferred activities does not accurately represent the day and reduces the child's trust in it. Including preferred activities in the schedule is essential for the tool to function as a reliable predictor of the day.
For educators who want to go deeper into what genuine autism support looks like in a school setting, the On the Spectrum podcast with Sonia Chand covers these practical, real-world topics in honest and accessible conversations that are valuable for educators as well as families.
Listen to the On the Spectrum podcast here and find the insights that help you support autistic students more effectively in your classroom.
Visual Schedules for Autism and Transitions
Transitions are one of the most reliably difficult aspects of daily life for autistic individuals, and visual schedules for autism are one of the most effective tools for reducing transition-related distress.
The distress autistic people experience around transitions is not primarily about the activity that is ending or the activity that is beginning. It is about unpredictability. The autistic nervous system experiences unexpected change as a threat, and the anxiety that follows is a genuine threat response rather than willful non-compliance.
A visual schedule for autism addresses this directly by making the next activity visible before the transition begins. The child who can see that outdoor play is followed by snack, which is followed by circle time, is experiencing a fundamentally different psychological situation than the child who never knows what is coming next.
For autistic children who are particularly demand-avoidant, combining the visual schedule for autism with the indirect language approaches covered in the pathological demand avoidance language to use post can significantly improve transition compliance and reduce the distress associated with necessary routine changes.
Common Mistakes With Visual Schedules for Autism
Even well-intentioned implementation of a visual schedule for autism can fall short if some common mistakes are not avoided.
Making the schedule too complex: A visual schedule for autism that represents an entire day in minute-by-minute detail can be overwhelming rather than clarifying. Start with the key anchor points in the day and add detail gradually.
Not using it consistently: A visual schedule for autism that is only brought out during difficult moments rather than used consistently throughout the day loses its predictive function. The schedule needs to be a regular, reliable part of the routine rather than an emergency intervention.
Not updating it when changes occur: When the schedule genuinely needs to change, updating the visual schedule for autism and previewing the change with the child is essential. The schedule is only a reliable predictor if it actually reflects what is going to happen.
Removing the schedule too quickly: Many parents and educators introduce a visual schedule for autism and then remove it as soon as the child seems to have learned the routine. The schedule is not just a learning tool. It is an ongoing support that reduces the cognitive and anxiety load even for routines that are well established.
When a Visual Schedule for Autism Is Not Enough
A visual schedule for autism is a powerful tool but it is not a complete solution on its own.
When a visual schedule for autism does not seem to be helping, the most common reasons include the format not matching the child's current visual processing level, the schedule not being used consistently across environments and adults, the schedule not including enough preferred activities to be genuinely representative of the day, or the underlying anxiety or sensory load being too high for any single tool to address adequately.
In these cases, a visual schedule for autism is most effective as part of a broader support plan that also addresses communication, sensory needs, and the specific anxiety triggers that are driving the distress.
For a deeper understanding of how different autism support tools and strategies fit together into a comprehensive picture, the post onwhat is level 2 autism covers the kind of multi-domain support planning that complex autism profiles require.
Final Thoughts
A visual schedule for autism is not a complicated or expensive intervention. It is a straightforward, evidence-based tool that works by meeting the autistic brain where it actually is, providing the predictability, the visual processing support, and the independence that autistic individuals consistently benefit from.
Getting it right takes some thoughtfulness in design and consistency in implementation. But when those elements are in place, the difference a visual schedule for autism makes to daily functioning, transition compliance, and anxiety levels is real, measurable, and often significant.
Start simple. Stay consistent. And trust the research that has been building the evidence for this tool for decades.
Is Autism a Learning Disability? What Parents and Adults Need to Know
Is autism a learning disability is one of those questions that gets asked constantly and answered inconsistently, leaving parents and autistic adults more confused than when they started. Is autism a learning disability in the clinical sense? Is it a learning disability in the school system sense? And does the answer even matter practically for getting the right support?
It matters enormously. And the answer is more nuanced than a simple yes or no.
This post answers is autism a learning disability directly and completely, explains what both terms actually mean, covers where they overlap and where they do not, and gives parents and autistic adults the clarity they need to advocate effectively for the right support in the right settings.
Table of Contents
Is Autism a Learning Disability? The Direct Answer
What Is a Learning Disability?
What Is Autism?
Where Autism and Learning Disabilities Overlap
Where Autism and Learning Disabilities Differ
Is Autism a Learning Disability in the US Education System?
How Autism Affects Learning
Co-occurring Learning Disabilities in Autism
What This Means for Educational Support
FAQs
Final Thoughts
Is Autism a Learning Disability?
Is autism a learning disability? In the United States clinical and educational framework, no. Autism and learning disabilities are two separate categories. They can and frequently do co-occur in the same person, but autism is not classified as a learning disability and having an autism diagnosis does not mean a person has a learning disability.
Is autism a learning disability in the UK? This is where the terminology gets genuinely confusing, because in the UK the term learning disability is used to mean something significantly different from what it means in the US. In the UK, learning disability refers to what Americans would call intellectual disability, a significant limitation in intellectual functioning and adaptive behavior. In the US, a learning disability refers specifically to neurological conditions that affect how a person processes information in specific academic areas, such as dyslexia, dysgraphia, or dyscalculia, without necessarily affecting overall intelligence.
Is autism a learning disability therefore depends significantly on which country's framework and which definition of the term you are working within, which is part of why the question generates so much confusion.
This post uses the US definition throughout unless otherwise specified.
What Is a Learning Disability?
Before going deeper into is autism a learning disability, it is worth being precise about what a learning disability actually means in the US context.
In the United States, a learning disability is a neurological condition that affects how the brain processes, stores, and communicates information in specific academic domains. Learning disabilities do not reflect overall intelligence. A person can have a high IQ and significant learning disabilities simultaneously.
The most commonly recognized learning disabilities include:
Dyslexia, which affects reading and language processing
Dysgraphia, which affects writing and fine motor coordination for written tasks
Dyscalculia, which affects mathematical processing and number sense
Auditory processing disorder, which affects how the brain processes sounds
Language processing disorder, which affects understanding and producing language
What these conditions share is that they represent a significant discrepancy between overall cognitive ability and performance in specific academic areas, driven by differences in how the brain processes specific types of information.
Under the Individuals with Disabilities Education Act, known as IDEA, specific learning disability is one of the thirteen disability categories that can qualify a child for special education services. Autism is a separate category under IDEA.
What Is Autism?
Is autism a learning disability requires equal clarity about what autism actually is.
Autism, formally known as Autism Spectrum Disorder or ASD, is a neurodevelopmental condition characterized by differences in social communication, sensory processing, and restricted or repetitive patterns of behavior and interests. It is present from birth and it is lifelong.
Autism does not inherently involve difficulties in specific academic processing areas in the way that learning disabilities do. Autism involves a broader neurodevelopmental profile that affects social communication, sensory experience, and behavioral patterns across all of life, not just in academic domains.
Intellectual ability in autism spans the full range from significant intellectual disability to exceptional cognitive gifts. Many autistic people are highly intelligent academically. Others have average intelligence. Some have intellectual disabilities that affect learning broadly. None of these variations are definitional features of autism itself.
For a comprehensive look at the relationship between autism and intellectual ability specifically, the post onis autism an intellectual disability covers this distinction in full detail.
Where Autism and Learning Disabilities Overlap
While is autism a learning disability has a clear no answer in the US clinical framework, autism and learning disabilities overlap in several practically important ways.
They can co-occur: Research consistently shows that learning disabilities occur at higher rates in autistic individuals than in the general population. Studies suggest that between 30 and 50 percent of autistic individuals have at least one co-occurring specific learning disability. Dyslexia and dysgraphia are particularly commonly co-occurring with autism.
They both affect learning: Both autism and learning disabilities can significantly affect how a person learns, though through different mechanisms. Autism affects learning through social communication differences, sensory processing differences, and executive functioning challenges. Learning disabilities affect learning through specific processing difficulties in defined academic domains.
They both qualify for educational support: Both autism and specific learning disabilities can qualify children for Individualized Education Programs under IDEA and for accommodations under Section 504 of the Rehabilitation Act. When they co-occur, educational planning needs to address both profiles.
They are both neurodevelopmental: Both autism and learning disabilities are classified as neurodevelopmental conditions, meaning they originate in differences in brain development during the early years of life and are present from birth.
Where Autism and Learning Disabilities Differ
Understanding where autism and learning disabilities differ is just as important as understanding where they overlap.
Scope: Learning disabilities affect specific academic processing areas while leaving other areas of cognitive functioning intact. Autism is a broader neurodevelopmental profile that affects social communication, sensory processing, and behavioral patterns across all domains of life, not just academic ones.
Social communication: Social communication differences are a core defining feature of autism and are not a feature of learning disabilities. A person with dyslexia, for example, does not necessarily experience any social communication difficulties at all.
Sensory processing: Significant sensory processing differences are characteristic of autism and are not part of the definition of learning disabilities.
Intelligence: Specific learning disabilities are defined partly by the presence of average or above average intelligence alongside specific processing difficulties. Autism is not defined by any particular level of intelligence and occurs across the full cognitive range.
Is Autism a Learning Disability in the US Education System?
In the US education system, is autism a learning disability in terms of how it is classified under federal law? No.
Under IDEA, autism is listed as one of thirteen separate disability categories that can qualify a child for special education services. Specific learning disability is a separate category. A child can qualify for special education under the autism category, the specific learning disability category, or both, if both profiles are present and both affect educational functioning.
This matters practically because the category under which a child is identified can affect what services and supports are made available to them. A child identified only under specific learning disability may not receive the social communication support, sensory accommodation, and behavioral support that an autism identification would prompt. A child identified only under autism may not receive the specific academic intervention that a learning disability identification would prompt.
When both autism and learning disabilities are present, advocating for identification and support under both categories is often the most effective approach for ensuring the child receives comprehensive educational support.
How Autism Affects Learning
Even though is autism a learning disability has a no answer in the US clinical framework, autism absolutely does affect learning in ways that are practically significant in educational settings.
Autism affects learning through several specific mechanisms:
Executive functioning: Many autistic individuals experience challenges with executive functioning including planning, organization, task initiation, working memory, and cognitive flexibility. These challenges can significantly affect academic performance independently of any specific learning disability.
Sensory processing: Sensory sensitivities can make the physical environment of a classroom genuinely difficult to learn in. Fluorescent lighting, background noise, and physical proximity to other students can all create a sensory load that significantly reduces the cognitive resources available for learning.
Social communication: The social dimension of learning, including group work, classroom discussion, and teacher-student interaction, can be significantly more demanding for autistic students than for neurotypical peers, creating an additional cognitive and emotional load that affects academic performance.
Anxiety: High rates of anxiety in autistic individuals, driven by social demands, sensory environment, and the unpredictability of school settings, significantly affect the ability to access learning even when cognitive ability is intact.
None of these are specific learning disabilities in the clinical sense. But all of them affect learning in ways that require educational accommodation and support.
Navigating the school system and understanding which of these factors are affecting your child's learning is genuinely complex, and having the right support alongside that navigation makes a real difference.
Dropped in a Maze by Sonia Chand is the book that helps families make sense of the autism journey, including the educational piece, in a way that is honest, practical, and grounded in real experience rather than clinical abstraction.
Co-occurring Learning Disabilities in Autism
Because co-occurring learning disabilities are common in autism, understanding how to identify and address them is a practically important part of comprehensive autism support.
Research published in the Journal of Learning Disabilities found that autistic children showed significantly higher rates of reading difficulties, including dyslexia, than the general population, with estimates suggesting that between 20 and 50 percent of autistic children may have co-occurring reading difficulties.
Dysgraphia, which affects written expression, is also commonly co-occurring with autism and is frequently underidentified because the writing difficulties are attributed to the autism rather than being recognized as a separate and specifically addressable condition.
When a learning disability co-occurs with autism, it requires targeted intervention specific to the learning disability alongside the broader autism support. Addressing the autism alone will not resolve a specific learning disability, and addressing only the learning disability will not address the broader autism support needs.
A comprehensive educational assessment that specifically looks for learning disabilities alongside the autism profile is therefore an important step for any autistic child who is struggling academically beyond what would be expected from the autism alone.
For parents navigating the process of getting their child properly assessed, The On the Spectrum podcast with Sonia Chand covers the real, practical challenges of navigating educational systems as an autism family, with honest conversations that give you the information and the community to keep going when the system makes it hard.
Listen to the On the Spectrum podcast here and find the support that helps you advocate more effectively for your child's educational needs.
What This Means for Educational Support
The practical implications of is autism a learning disability for educational support planning are significant.
An autistic child without co-occurring learning disabilities needs educational support that addresses social communication differences, sensory accommodation, executive functioning support, and behavioral regulation, but does not necessarily need the specific academic intervention that a learning disability would require.
An autistic child with co-occurring learning disabilities needs all of the above plus targeted intervention for the specific learning disability. Dyslexia-specific reading intervention for an autistic child with dyslexia, for example, is genuinely different from and in addition to the broader literacy support that autism alone might require.
Getting this right in an IEP requires a comprehensive assessment that specifically looks for both profiles and educational planning that addresses both clearly and specifically. Advocating for that level of comprehensive assessment is one of the most important things parents can do for an autistic child who is struggling academically.
FAQs
Is autism a learning disability?
No. In the US clinical and educational framework, autism and learning disabilities are separate categories. They can co-occur but autism is not classified as a learning disability.
Can you have autism and a learning disability?
Yes. Research suggests between 30 and 50 percent of autistic individuals have at least one co-occurring specific learning disability.
Does autism affect learning?
Yes, through executive functioning challenges, sensory processing differences, social communication demands, and anxiety, though these are distinct from specific learning disabilities in the clinical sense.
Should my autistic child be assessed for learning disabilities? I
f your child is struggling academically beyond what would be expected from their autism alone, a comprehensive assessment specifically looking for co-occurring learning disabilities is strongly recommended.
Does having autism mean my child will struggle at school?
Not necessarily, but autism does create specific challenges in educational settings that require appropriate accommodation and support to address effectively.
What is the difference between a learning disability and a learning difficulty?
In the US, learning disability is the clinical term for specific processing difficulties. In the UK, learning difficulty is used for similar conditions while learning disability refers to intellectual disability.
Final Thoughts
Is autism a learning disability? No, not in the US clinical framework. But that no answer should not be taken to mean that autism does not significantly affect learning, because it does, through a range of mechanisms that require real and specific educational accommodation.
And when learning disabilities co-occur with autism, which they do more often than most people realize, those learning disabilities deserve their own targeted identification and support alongside the broader autism support plan.
Getting this distinction right matters practically. It affects what assessments are requested, what support is put in place, and whether the autistic child or adult gets the full picture of what they need rather than a partial answer to an incomplete question.
References:
NHS. What is autism? [Internet]. Available from: https://www.nhs.uk/conditions/autism/what-is-autism/
Vallejo M. Is Autism a Learning Disability? [Internet]. Mental Health Center Kids; 2025 Jan 27. Available from: https://mentalhealthcenterkids.com/blogs/articles/is-autism-a-learning-disability
Congressional Research Service. The Individuals with Disabilities Education Act: A Comparison of State Eligibility Criteria [Internet]. Report R46566. 2020 Oct 12. Available from: https://www.congress.gov/crs-product/R46566
Knight C, Lowthian E, Jenks E, Jones C. The relationship between dyslexia, autism, and academic outcomes: longitudinal analysis of population-level education and health data. Oxf Rev Educ. 2025. Available from: https://doi.org/10.1080/03054985.2025.2590464
Academics West. A Parent's Guide to Qualifying Disabilities Under the IDEA [Internet]. 2026 Jan 30. Available from: https://academicswest.com/a-parents-guide-to-qualifying-disabilities-under-the-idea/

Is Autism Always Noticeable? What Most People Get Wrong
Is autism always noticeable? The short answer is no, and the gap between what most people expect autism to look like and what it actually looks like in many individuals is one of the most significant reasons autism goes unidentified for so long in so many people.
Is autism always noticeable is a question that matters for parents watching their child and wondering if what they are seeing is significant enough to pursue, and for adults who have spent years feeling different without ever having a name for why. In both cases, the assumption that autism is always visible and always obvious is one of the most persistent and most damaging myths in the public understanding of this condition.
This post unpacks what autism actually looks like across the full spectrum, why it is so often invisible, and what that invisibility costs the people living with it.
Table of Contents
Is Autism Always Noticeable? The Direct Answer
Where the Visible Autism Stereotype Comes From
What Invisible Autism Actually Looks Like
Why Autism Is Not Always Noticeable in Girls
The Role of Masking in Making Autism Invisible
Is Autism Always Noticeable at School
Is Autism Always Noticeable in Adults
The Cost of Invisible Autism
When Autism Becomes More Visible
FAQs
Final Thoughts
References
Is Autism Always Noticeable? The Direct Answer
Is autism always noticeable? No. Autism is not always noticeable, and in many cases it is actively invisible to the people closest to the autistic person, including parents, teachers, partners, and sometimes even the autistic person themselves.
The reason for this is not that the autism is less real or less impactful in these cases. It is that autism presents in an enormous range of ways, and many of those presentations do not match the image that most people carry in their heads when they think about what autism looks like. The child who is nonverbal, who rocks and flaps and does not make eye contact, is visible. The child who talks constantly about one specific topic, who manages socially by watching and copying peers, who holds it together at school and falls apart at home is far less visible. Both are autistic.
Is autism always noticeable depends entirely on which presentation you are looking at, which environment you are observing, and what you have been taught to look for.
Where the Visible Autism Stereotype Comes From
Understanding why people ask is autism always noticeable requires understanding where the stereotype of visible autism came from in the first place.
Early autism research, from the 1940s through to the 1990s, was conducted almost entirely on male children with significant support needs. The diagnostic criteria were developed from observations of this specific population, which meant the resulting picture of autism was dominated by the most visible and most impactful presentations. Autism became associated, in the public mind and in much of the clinical mind, with significant intellectual disability, absent or very limited speech, and highly visible repetitive behaviors.
As diagnostic criteria broadened and awareness grew, a much wider and more diverse population of autistic individuals began to be identified. Many of them looked almost nothing like the original stereotype. But the stereotype persisted in public consciousness long after the clinical picture had changed, and it continues to shape who gets identified, who gets believed, and who gets left without support.
What Invisible Autism Actually Looks Like
Is autism always noticeable in the people we might least expect? Absolutely not, and understanding what invisible autism looks like helps both parents and adults recognize it in themselves or their children.
Invisible autism often looks like:
A child who is highly verbal, academically capable, and appears to cope at school but who comes home and falls apart completely
A child who watches peers carefully and copies their behavior with enough success that the underlying difficulty is not visible from the outside
An adult who has built a functional life but who finds it exhausting in ways they cannot fully explain to anyone around them
Someone who is described as quirky, intense, or a bit different but who has never been flagged as autistic because they manage well enough in structured environments
A person whose sensory sensitivities, rigid routines, and social exhaustion are attributed to personality traits, anxiety, or simply being an introvert
None of these presentations are unusual. They are in fact among the most common ways autism presents across the population once you move beyond the most visible end of the spectrum.
Why Autism Is Not Always Noticeable in Girls
Is autism always noticeable in girls? Even less so than in boys, and this is one of the most significant and best-documented sources of missed diagnosis in the autism community.
Girls with autism are significantly more likely to mask their autistic traits than boys. They observe social behavior carefully, imitate it, and use their social awareness to compensate for the genuine social communication differences underneath. The result is a presentation that can look like shyness, social anxiety, or simply being quiet rather than autism.
Research found that autistic females showed significantly greater camouflaging of autistic traits than autistic males, with the degree of camouflaging contributing directly to delayed diagnosis and increased mental health burden.
Is autism always noticeable in the girls sitting quietly in the back of classrooms, managing socially with enormous effort, and coming home completely depleted? Almost never. And the cost of that invisibility is measured in years of missed support, compounding anxiety, and a quiet sense of being wrong about themselves that most of these girls carry into adulthood before they ever receive a diagnosis.
This is one of the conversations that comes up regularly on the On the Spectrum podcast with Sonia Chand, where real, honest discussions about the autism journey, including who gets seen and who does not, happen in a way that is genuinely useful for families and individuals trying to navigate this.
Listen to the On the Spectrum podcast here and find the conversations that help you see autism more clearly, in all the forms it actually takes.
The Role of Masking in Making Autism Invisible
Is autism always noticeable when the autistic person is actively working to make it invisible? This is the reality for a significant proportion of autistic people, and it is called masking.
Masking is the conscious or semi-conscious suppression of autistic traits in order to appear more neurotypical. It involves forcing eye contact that feels uncomfortable, using rehearsed scripts for social interactions, suppressing stimming in public, and performing calm when internally dysregulated. For many autistic people, masking becomes so automatic over time that they themselves are not fully aware they are doing it.
Masking is directly relevant to the question of is autism always noticeable because it is one of the primary mechanisms through which autism becomes invisible, both to observers and sometimes to the autistic person themselves.
Research identified masking as a significant factor in delayed autism diagnosis and found it was associated with substantially higher rates of depression, anxiety, and suicidal ideation in autistic individuals, particularly women.
The cost of masking is high and it is real, and understanding it is one of the most important parts of understanding why autism is not always noticeable.
If you are an autistic adult who has spent years masking and is now starting to understand what that has cost you, Dropped in a Maze by Sonia Chand speaks directly to that experience. It is the honest account of navigating an autism journey without a clear map, and it captures the exhaustion of going unseen in a way that very few books manage.
Get your copy of Dropped in a Maze here and find the words for an experience you may have been carrying alone for a very long time.
Is Autism Always Noticeable at School
Is autism always noticeable in a school environment? For many autistic children, school is precisely the place where autism is least visible, because school provides the structured, predictable environment that autistic children often manage best.
Many autistic children hold themselves together through the school day using enormous amounts of cognitive and emotional energy. They follow the routine, they stay in their seat, they do their work, and they appear to be managing. Teachers who do not know what to look for, and who are working with large classes under significant pressure, may see only the surface level of functioning rather than the effort underneath it.
Is autism always noticeable at home? Much more so, because home is where the mask comes off. The child who appeared fine at school is explosive, exhausted, or completely shut down at home. This pattern, doing well at school and falling apart at home, is one of the most consistent signs of invisible autism in children and one that is frequently misunderstood by both parents and schools.
For parents who are navigating this exact pattern and trying to figure out whether what they are seeing warrants a formal evaluation, the post on how to test for autism covers the entire assessment process from first concern through to diagnosis.
Is Autism Always Noticeable in Adults
Is autism always noticeable in adults? Even less so than in children, for several compounding reasons.
By adulthood, many autistic people have spent decades building compensatory strategies for the things that do not come naturally. They have developed scripts for social situations, careers that play to their strengths, and routines that reduce the daily demand on their nervous system. The autism is still there, shaping every aspect of how they experience the world, but the compensatory scaffolding around it can make it almost entirely invisible to people who do not know what they are looking for.
Many adults discover they are autistic for the first time only after a child receives a diagnosis and the parent recognizes their own childhood in the child's traits. Others get there after years of therapy for anxiety, depression, or burnout that never quite got to the root of what was actually driving those experiences.
Is autism always noticeable when an autistic adult walks into a room? Almost never. And for the adult who has spent a lifetime not understanding themselves, that invisibility has a cost that is real and deep and deserves real and skilled support.
Coaching with Sonia offers exactly that, personalised, neurodivergent-affirming support for adults who are finally putting the pieces together and building a life that works for their actual brain rather than the neurotypical one they have been performing for decades.
Book a coaching session with Sonia here and start getting support that finally understands how you are actually wired.
The Cost of Invisible Autism
Is autism always noticeable is ultimately a question about who gets seen, and the answer has direct consequences for who gets help.
When autism is not noticeable, it does not get identified. When it does not get identified, the autistic person does not receive the understanding, accommodation, and support they need. The mental health consequences of that gap are significant and well-documented: higher rates of anxiety, depression, burnout, and suicidal ideation in autistic individuals who are identified late or not at all.
The cost of invisible autism is also relational. Years of not understanding why social situations feel so hard, why relationships struggle in ways that are difficult to explain, and why the exhaustion never seems to lift takes a toll that persists even after a diagnosis eventually arrives.
For a deeper understanding of what happens when autism goes without the right support, the post on if autism is left untreated covers the research and the real-world consequences in full.
When Autism Becomes More Visible
Is autism always noticeable even in people who usually mask effectively? There are specific circumstances where autism becomes more visible even in people who have compensated effectively for years.
These include periods of significant stress or change, major life transitions such as starting university or a new job, physical illness that depletes the energy available for masking, periods of autistic burnout, and environments that are significantly more sensory or socially demanding than usual.
Understanding this helps explain why autism sometimes seems to appear suddenly in people who previously appeared to be managing well. The autism was always there. The circumstances simply changed enough that the usual compensatory strategies could no longer hold.
FAQs
Is autism always noticeable?
No. Many autistic people, particularly women, late-diagnosed adults, and those who mask effectively, present in ways that are not visibly recognizable as autism.
Can someone be autistic and appear completely typical?
Yes. Effective masking, compensation strategies, and structured environments can make autism essentially invisible to outside observers.
Can autism become more visible over time?
Yes. During periods of significant stress, burnout, or major life transitions, autism often becomes more visible even in people who have compensated effectively for years.
Is invisible autism less severe than visible autism?
No. The internal experience and impact of invisible autism can be just as significant as more visible presentations. Invisible autism often involves intense masking that has significant mental health consequences.
Can a doctor miss autism because it is not noticeable?
Yes. This happens regularly, particularly for women, adults, and individuals who present outside the most visible stereotype of autism.
What should I do if I suspect autism but it is not obviously noticeable?
Document specific behaviors across multiple settings, trust your observations, and request a formal evaluation from a clinician with specific experience in the less visible presentations of autism.
Final Thoughts
Is autism always noticeable? No. And that simple answer carries enormous implications for the millions of autistic people who have gone unidentified, unsupported, and unseen because the people around them were looking for something that did not match what they actually were.
Autism is visible when we know what to look for. It is visible in the child who holds it together all day and falls apart at home. It is visible in the adult who is exhausted in ways they cannot fully explain. It is visible in the years of anxiety, depression, and burnout that accumulate when the right framework and the right support never arrive.
Learning to see autism in all its forms, not just the most obvious ones, is one of the most important things we can do for the autistic people in our lives and for the autistic people who do not yet know that is what they are.
References:
Augie. The diagnosis story [Internet]. Autistic Pride Day; 2025 Jan 14. Available from: https://autisticprideday.org/diagnosis-history/
Wood-Downie H, Wong B, Kovshoff H, Mandy W, Hull L, Hadwin JA. Sex/Gender Differences in Camouflaging in Children and Adolescents with Autism. J Autism Dev Disord. 2021;51(4):1353-1364. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7985051/
Conde-Pumpido-Zubizarreta S, Cruz S, Pozo-Rodríguez M, Suárez-Rama JJ, Díaz-Hernández A, Carracedo A, Tubío-Fungueiriño M, Fernández-Prieto M. The association between autism, camouflaging and anxiety with suicidal ideation in women. Front Psychol. 2026;16:1685845. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12879100/
UNICEF. Autism symptoms: Common signs of ASD in children [Internet]. 2025 Apr 2. Available from: https://www.unicef.org/eca/stories/autism-symptoms-common-signs-asd-children
Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). What are the symptoms of autism? [Internet]. Last reviewed 2025 Dec 23. Available from: https://www.nichd.nih.gov/health/topics/autism/conditioninfo/symptoms

If Autism Is Left Untreated: What Actually Happens and Why It Matters
If autism is left untreated is one of the most searched questions about autism, and it carries a weight that most other search queries do not. Behind it is usually a parent who is scared, or an adult who is starting to wonder whether years of struggling without a diagnosis has quietly cost them more than they realized.
The honest answer to what happens if autism is left untreated is not simple, because autism is not a single condition with a single trajectory. What happens depends enormously on the individual, their specific profile, their environment, and what kind of support was or was not available to them. But the research is clear enough on several key points that it is worth addressing directly and honestly, without either minimizing the real consequences or catastrophizing in ways that help nobody.
This post covers what the research actually says about what happens if autism is left untreated, what untreated really means in this context, and what genuinely changes when the right support finally arrives.
Table of Contents
What Does Untreated Actually Mean in Autism
If Autism Is Left Untreated: Mental Health Consequences
If Autism Is Left Untreated: Communication and Social Development
If Autism Is Left Untreated: Education and Employment
If Autism Is Left Untreated: Relationships and Isolation
If Autism Is Left Untreated: Physical Health
The Difference the Right Support Makes
It Is Never Too Late
FAQs
Final Thoughts
What Does Untreated Actually Mean in Autism
Before going further it is worth being clear about what untreated actually means in the context of autism, because the word treatment carries different implications here than it does in the context of a disease or infection.
Autism is not a disease. It cannot be cured and it does not need to be. When people ask what happens if autism is left untreated, what they are really asking is: what happens when an autistic person goes without the understanding, accommodation, support, and tools they need to navigate a world that was not designed for their neurology.
Untreated in autism means unidentified, unsupported, and unaccommodated. It means a child growing up without anyone around them understanding why things are hard, without the right educational support, without the communication tools they need, and without the framework to make sense of their own experience. It means an adult spending decades wondering why they are different, why relationships are so hard, and why they are so exhausted by things that seem effortless for everyone else.
When framed that way, the question of what happens if autism is left untreated becomes both clearer and more urgent.
If Autism Is Left Untreated: Mental Health Consequences
The most consistently documented consequence of autism being left untreated is significant mental health impact.
Research published in the journal Autism in Research found that autistic individuals who are undiagnosed or who receive a late diagnosis report significantly higher rates of anxiety and depression than those identified and supported earlier..
This is not a coincidence. If autism is left untreated, the autistic person spends years, sometimes decades, trying to function in an environment that does not accommodate them, masking their natural responses, absorbing repeated messages that they are too much, too sensitive, too rigid, or simply not trying hard enough. That accumulated experience has a real and measurable cost.
Anxiety and depression in unidentified autism are not separate conditions that happen to occur alongside autism. They are frequently the direct result of what happens when autism is left untreated and the gap between what the autistic person needs and what they receive goes unaddressed year after year.
If Autism Is Left Untreated: Communication and Social Development
For children in particular, if autism is left untreated during the critical early developmental window, communication and social development are among the most significantly affected areas.
The brain is most neuroplastic in the earliest years of life. When autism is identified early and the right communication support is put in place during that window, children develop stronger functional communication skills than they would develop without it. When autism is left untreated during that same window, the gaps between the autistic child and their neurotypical peers in both communication and social skill development tend to widen rather than close on their own.
This does not mean that communication development stops or that social skills cannot be built later. Many autistic individuals make significant gains in both areas throughout childhood, adolescence, and adulthood. But the research is consistent that earlier support produces better outcomes, and the absence of early support leaves gaps that take more effort to address later.
For children who are nonverbal or minimally verbal, if autism is left untreated the consequences for communication are particularly significant because the window for establishing an alternative communication channel, such as AAC, is also most effective in the early years.
The post on early autism detection covers in detail why early identification and early support make such a measurable difference, and is worth reading alongside this one.
If Autism Is Left Untreated: Education and Employment
If autism is left untreated, the consequences ripple through education and into adult employment in ways that compound over time.
In school, an autistic child without identification or support is typically expected to meet the same academic and behavioral standards as neurotypical peers, without the accommodations that would allow them to actually demonstrate what they know. Sensory overload goes unaddressed. Executive functioning difficulties go unsupported. Social misunderstandings accumulate and affect both peer relationships and teacher relationships. Many autistic children without identification are labeled as lazy, difficult, disruptive, or underachieving, when the reality is that they are working significantly harder than anyone around them realizes just to get through the day.
In employment, the picture for adults if autism is left untreated is similarly challenging. Research from Drexel University's Autism Institute found that autistic adults have among the lowest employment rates of any disability group, with many struggling to maintain employment not because of lack of ability but because of the absence of accommodations, the demands of masking, and the social complexity of workplace environments that were not designed for autistic brains.
Dropped in a Maze by Sonia Chand is one of the most honest accounts of what it looks like to navigate the autism journey without a clear map, and it is exactly the kind of reading that helps families and autistic individuals understand not just what support is needed but how to find their way through a system that does not always make it easy.
Get your copy of Dropped in a Maze here
If Autism Is Left Untreated: Relationships and Isolation
If autism is left untreated, relationships are one of the areas where the impact accumulates most quietly and most painfully.
Without a framework for understanding their own social communication differences, autistic people often experience repeated relationship failures that they cannot explain or prevent. Friendships that start well and then inexplicably fall apart. Romantic relationships that struggle under the weight of unmet communication needs. Family relationships strained by years of being misunderstood. The absence of a diagnosis means the absence of a shared language for understanding what is actually happening in these relationships and what would genuinely help.
Social isolation is one of the most consistent findings in research on untreated autism across the lifespan. And social isolation, in turn, significantly worsens the mental health consequences already described above.
If you are navigating these relationship and communication challenges and looking for practical, personalised support built around your actual neurology, coaching with Sonia is exactly the kind of help that makes a real difference.
Book a coaching session with Sonia here and start building the communication tools and social confidence that change how relationships actually feel.
If Autism Is Left Untreated: Physical Health
Physical health is an often overlooked area of what happens if autism is left untreated, but the research here is worth taking seriously.
Autistic individuals have higher rates of several physical health conditions including gastrointestinal disorders, sleep disorders, and epilepsy. When autism is left untreated and unidentified, these co-occurring conditions are frequently also missed, misattributed, or managed inadequately because the underlying autism context that would help clinicians understand them is not recognized.
Sleep disorders in particular have a significant downstream impact on every other area of functioning including mental health, cognitive performance, emotional regulation, and daily functioning. When autism is left untreated, sleep issues are often attributed to behavioral causes rather than the neurological differences driving them, leading to interventions that do not address the actual problem.
Research published in the journal Sleep Medicine Reviews has found that sleep disturbances affect between 40 and 80 percent of autistic individuals and that addressing them has significant positive effects on daytime functioning, behavior, and quality of life.

The Difference the Right Support Makes
Understanding what happens if autism is left untreated is most useful when paired with an equally clear picture of what changes when the right support is finally in place.
When autism is identified and supported appropriately, anxiety decreases because the autistic person finally has a framework for understanding their own experience. Communication improves because the right tools and strategies are available. Relationships become easier to navigate because there is shared language for what is actually happening. Employment becomes more sustainable because accommodations can be requested and implemented. And the years of accumulated self-blame, shame, and confusion begin to give way to something more accurate and more compassionate.
The On the Spectrum podcast with Sonia Chand covers exactly these kinds of real, honest conversations about what the journey from untreated to genuinely supported looks like, with guests who have navigated it themselves and with the kind of practical insight that makes a real difference.
Listen to the On the Spectrum podcast here and find the conversations that make the journey feel less impossible.
The right support does not undo the years that passed without it. But it can genuinely change what the years ahead look like, and that is worth everything.
It Is Never Too Late
One of the most important things to say about if autism is left untreated is that the damage is not permanent and it is never too late for the right support to make a genuine difference.
Adults who are diagnosed later in life consistently report that the diagnosis, even when it comes decades after it should have, changes things. The framework it provides for understanding a lifetime of experiences has real and lasting value. The support it opens access to, whether that is workplace accommodations, appropriate therapy, or coaching built around actual autistic neurology, makes a measurable difference to quality of life regardless of when it arrives.
For autistic adults who are recognising themselves in this post and wondering where to start, coaching with Sonia offers exactly the kind of personalised, neurodivergent-affirming support that meets you exactly where you are right now.
FAQs
What happens if autism is left untreated?
Without identification and support, autistic individuals face significantly higher rates of anxiety, depression, social isolation, educational underachievement, and employment difficulties.
Can autism get worse if left untreated?
Autism itself does not worsen, but the secondary consequences including mental health, relationships, and life opportunities are significantly worse without appropriate support.
Is it too late to get support for autism as an adult?
No. Support at any age makes a meaningful difference to quality of life, and adult diagnosis opens access to accommodations and understanding that were previously unavailable.
What is the most important thing to do if autism has gone unidentified?
Pursue formal assessment, access appropriate support as soon as possible, and connect with community. The clarity that comes from identification, even late, changes things meaningfully.
Can the effects of untreated autism be reversed?
Many of the secondary consequences can be significantly improved with the right support. The earlier the support arrives the better, but meaningful improvement is possible at any age.
Final Thoughts
If autism is left untreated, the consequences are real, they are documented, and they compound over time. But they are not inevitable, and they are not permanent.
The difference between an autistic person who goes without support and one who receives the right support at the right time is not a difference in the autism itself. It is a difference in whether the world around them made room for who they actually are.
That room can be made at any point. And making it, however late it comes, matters.
References:
Autism Research Institute. Treating Sleep Disorders [Internet]. Last updated September 2024. https://autism.org/treating-sleep-disorders/
Belenguer LM, Cabrera TDLC, Arboledas GP. Sleep Characteristics in Children and Adolescents With Autism Spectrum Disorder. J Sleep Med. 2025 Aug;22(2):49-62.https://www.e-jsm.org/journal/view.php?number=415
Roux AM, Shattuck PT, Rast JE, Rava JA, Anderson KA. National Autism Indicators Report: Transition into Young Adulthood. Philadelphia, PA: Life Course Outcomes Research Program, A.J. Drexel Autism Institute, Drexel University; 2015.https://drexel.edu/~/media/Files/autismoutcomes/publications/LCO%20Fact%20Sheet%20Employment.ashx

Pathological Demand Avoidance Language to Use: A Practical Guide for Teachers and Educators
Pathological demand avoidance language to use is one of the most searched and most practically urgent questions for anyone working with a child who has a PDA profile. You have probably already learned that standard classroom management approaches do not work with these children. What you may not yet have is a clear, specific, evidence-informed alternative to replace them with.
The right pathological demand avoidance language to use is not about being soft, lowering expectations, or abandoning structure entirely. It is about understanding what is actually driving the avoidance and choosing words that work with the child's nervous system rather than triggering it further. The difference in outcome between getting the language right and getting it wrong can be the difference between a child who participates and one who shuts down entirely.
This post covers the theory behind why language matters so profoundly in pathological demand avoidance, the specific pathological demand avoidance language to use in real classroom situations, and the words and phrases to avoid entirely.
Table of Contents
Why Language Matters So Much in Pathological Demand Avoidance
The Core Principle Behind Pathological Demand Avoidance Language to Use
Pathological Demand Avoidance Language to Use: Indirect Requests
Pathological Demand Avoidance Language to Use: Offering Genuine Choice
Pathological Demand Avoidance Language to Use: Collaborative Framing
Pathological Demand Avoidance Language to Use: Removing Yourself as the Authority
Language to Avoid With PDA Children
Pathological Demand Avoidance Language in Conflict Moments
FAQs
Final Thoughts
Why Language Matters So Much in Pathological Demand Avoidance
Before getting into specific pathological demand avoidance language to use, it helps to understand why language has such an outsized impact on children with this profile compared to neurotypical children or even other autistic children.
Pathological demand avoidance is driven by extreme anxiety about loss of control and autonomy. When a demand is made, the child's nervous system registers it as a threat, not an inconvenience. The fight, flight, or freeze response activates, and from that state, compliance is neurologically very difficult rather than simply undesirable.
What this means practically is that the words used to make a request carry more neurological weight for a child with PDA than for most other children. A direct instruction that would be processed neutrally by a neurotypical child can trigger a full threat response in a child with PDA, not because the child is being deliberately difficult but because their nervous system is responding to the directness itself as a source of danger.
This is why pathological demand avoidance language to use consistently centers on reducing the felt experience of being controlled, because reducing that experience reduces the anxiety, and reducing the anxiety is what allows the child to actually engage.
For a full understanding of what pathological demand avoidance is and how it differs from other autism profiles and from oppositional defiant disorder, the post onpathological demand avoidance vs oppositional defiant disorder covers the distinction in depth and is essential reading before applying any language strategy in the classroom.
Language to use
The Core Principle Behind Pathological Demand Avoidance Language to Use
Every piece of pathological demand avoidance language to use is built on one core principle: reduce the experience of external imposition without removing the necessary expectation.
This is not the same as having no expectations. It is about how expectations are communicated. The goal is to frame the necessary activity, the math worksheet, the transition to lunch, the putting away of materials, in a way that does not trigger the threat response that direct instruction creates.
The four main strategies for pathological demand avoidance language to use are indirect requests, genuine choice, collaborative framing, and removing yourself as the authority. Each one is covered in detail below with real classroom examples.
Pathological Demand Avoidance Language to Use: Indirect Requests
Indirect language is one of the most powerful tools in the pathological demand avoidance language to use toolkit. Rather than making a direct request, you wonder aloud, make an observation, or pose a question that creates an opening without issuing an instruction.
Instead of: Sit down and start your work. Try: I wonder if anyone around here is ready to take a look at today's task.
Instead of: You need to pack away your materials now. Try: It looks like it might nearly be time to start thinking about packing up.
Instead of: Stop talking and listen. Try: There might be something interesting coming up that someone wouldn't want to miss.
The indirect request removes the explicit demand while still communicating the expectation. For a child with pathological demand avoidance, this distinction is significant because the instruction is no longer being issued by an authority figure to them specifically. The demand has been depersonalized, and that reduction in perceived external control reduces the anxiety enough to allow participation.
Pathological Demand Avoidance Language to Use: Offering Genuine Choice
Choice is one of the most consistently effective elements of pathological demand avoidance language to use, but only when the choice is genuine. Offering a fake choice, where both options lead to the same outcome with no real agency, is often recognized immediately by children with PDA and can worsen the response.
Genuine choice in pathological demand avoidance language to use looks like offering real alternatives about how or when something happens, even when what needs to happen is not negotiable.
Instead of: You must complete this worksheet before break. Try: This worksheet needs to happen today. Do you want to start it now or after you have had five minutes to settle in?
Instead of: Come and join the group now. Try: The group is starting over there. Do you want to grab a chair and choose where you sit, or would you prefer to observe for a bit first?
Instead of: You have to do your reading today. Try: Reading is on the list for today. Would you rather do it at your desk or somewhere quieter?
Genuine choice communicates that the child has real agency within necessary structure, and that experience of agency directly reduces the anxiety that drives pathological demand avoidance.
Tired of figuring it all out alone? Coaching with Sonia gives you the tools, the clarity, and someone who genuinely gets it.
Pathological Demand Avoidance Language to Use: Collaborative Framing
Collaborative framing shifts the language from you need to do this to we are figuring this out together. It positions the adult as an ally rather than an authority issuing directives, which reduces the perceived threat significantly.
Instead of: You need to finish that before we move on. Try: Let us see if we can figure out how to get through this bit together.
Instead of: I need you to stop doing that. Try: I am trying to work out what would help right now. What do you think?
Instead of: This is the rule and you have to follow it. Try: I know this one is tricky. Can we think about how to make it work?
Research on collaborative problem solving approaches, including the work of Dr. Ross Greene whose Collaborative and Proactive Solutions model has been widely applied with behaviorally complex children. It has consistently shown that collaborative language produces better compliance and better relationship quality than authoritative instruction, particularly with children who are anxiety-driven rather than defiance-driven.
This connects directly to the broader point that understanding pathological demand avoidance as anxiety-driven rather than defiance-driven changes everything about how you respond. Navigating that shift in understanding as a parent or educator can feel overwhelming without the right support alongside it.
Dropped in a Maze by Sonia Chand is one of the most honest, practically grounded accounts of navigating a neurodivergent journey, and it is exactly the kind of reading that helps educators and families develop the kind of understanding that makes language shifts like these feel genuinely possible rather than just theoretical.
Get your copy of Dropped in a Maze here and build the foundation of understanding that makes real change possible in your classroom and beyond.
Dropped in a Maze by Sonia Chand
Pathological Demand Avoidance Language to Use: Removing Yourself as the Authority
One of the most effective categories of pathological demand avoidance language to use is language that removes the educator as the source of the demand entirely, attributing the expectation to an external rule, a necessity, or simply the nature of how things work.
Instead of: I am telling you that you need to stop. Try: The thing about this particular activity is that it needs to wrap up now so the next thing can happen.
Instead of: Because I said so. Try: It is one of those things that just needs to happen before we can move forward.
Instead of: You need to do what I ask. Try: This is one of the non-negotiable ones today, but how we get there is completely up to you.
This strategy is particularly useful because it takes the interpersonal power dynamic out of the equation. The child is not being controlled by a person. They are simply navigating a situation, and that subtle shift can be enough to reduce the threat response meaningfully.
Language to Avoid With PDA Children
Understanding pathological demand avoidance language to use also means knowing what to remove from your current vocabulary with these children.
Avoid:
You must, you need to, you have to
Because I said so
Everyone else is doing it
If you do not do this, then
You always, you never
I am not asking, I am telling you
That is not acceptable behavior
You need to calm down
All of these phrases either issue a direct demand, apply social pressure, or escalate the threat experience. Each one is likely to worsen rather than reduce the avoidance response in a child with pathological demand avoidance.
Pathological Demand Avoidance Language in Conflict Moments
When a child with PDA is already dysregulated, the pathological demand avoidance language to use changes again. The goal in a conflict moment is not to resolve the original demand but to reduce the threat experience enough that the nervous system can begin to regulate.
Useful language in conflict moments:
I can see this is really hard right now.
There is no rush. I am not going anywhere.
We do not have to sort this out right this minute.
You are not in trouble. I just want to understand.
What would help you feel safer right now?
None of these abandon the expectation. They simply pause the demand long enough to allow the nervous system to come down from the threat response, after which re-engagement becomes genuinely possible again.
If you are regularly navigating these moments and finding them exhausting, you are not alone. The On the Spectrum podcast with Sonia Chand covers exactly these kinds of difficult, real-world challenges around neurodivergent children in honest, practical conversations that are genuinely useful for educators as well as families.
FAQs
What is the best pathological demand avoidance language to use with a child who is already dysregulated?
Focus on reducing the threat experience first. Use language that communicates safety and removes time pressure before attempting to re-engage with the original expectation.
Does using indirect language mean I am letting the child get away with not doing what is expected?
No. The expectation remains. What changes is how it is communicated, in a way that reduces the anxiety response that prevents the child from being able to meet it.
Can these language strategies be used by teachers who are not specialists in autism?
Yes. The strategies are practical and applicable by any educator willing to shift their communication approach, though understanding the underlying reasons for pathological demand avoidance makes them significantly more effective.
How long does it take to see results from changing pathological demand avoidance language?
Results vary. Some children respond almost immediately to language changes. Others require a longer period of consistent low-demand communication before trust is established enough for engagement to improve.
Is pathological demand avoidance language to use different for younger versus older children?
The core principles are the same. The specific language needs to be adapted to developmental level, with simpler and more concrete indirect framing for younger children and more nuanced collaborative language for older children and teenagers.
Final Thoughts
Pathological demand avoidance language to use is not a magic script. It is a framework rooted in understanding what is actually driving the behavior and responding to that underlying driver rather than to the surface behavior itself.
When the language changes from controlling to collaborative, from direct to indirect, from authoritative to autonomous, the child's nervous system experiences less threat. Less threat means less anxiety. Less anxiety means less avoidance. And less avoidance means more genuine engagement with learning, with relationships, and with the world.
Getting there takes practice, consistency, and a willingness to unlearn communication habits that feel natural but that consistently backfire with this specific profile. It is worth every bit of that effort.
For more on what pathological demand avoidance is and how it differs from other profiles, read the complete post on pathological demand avoidance in autism and the post on pathological demand avoidance vs oppositional defiant disorder.
References:
O'Nions E, Gould J, Christie P, Gillberg C, Viding E, Happé F. Identifying features of 'pathological demand avoidance' using the Diagnostic Interview for Social and Communication Disorders (DISCO). Eur Child Adolesc Psychiatry. 2016 Apr;25(4):407-419. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4820467/
PDA North America. Declarative Language & PDA [Internet]. 2024. Available from: https://pdanorthamerica.org/wp-content/uploads/2024/01/Declarative-Language-PDA.pdf
PDA Society. PANDA as a Way In [Internet]. Last updated June 2026. Available from: https://www.pdasociety.org.uk/what-helps-guides/pda-approaches/panda-as-a-way-in/
Greene R, Winkler J. Collaborative & Proactive Solutions (CPS): A Review of Research Findings in Families, Schools, and Treatment Facilities. Clin Child Fam Psychol Rev. 2019 Dec;22(4):549-561. Available from: https://pubmed.ncbi.nlm.nih.gov/31240487/
Miller C. Pathological Demand Avoidance (PDA) in Kids [Internet]. Child Mind Institute. Last reviewed January 2026. Available from: https://childmind.org/article/pathological-demand-avoidance-in-kids/
Pathological Demand Avoidance vs Oppositional Defiant Disorder: What Is the Difference
Pathological demand avoidance vs oppositional defiant disorder is one of the most important distinctions a parent or adult can learn to make, because the two profiles can look almost identical on the surface while requiring completely different responses underneath. Getting this distinction wrong does not just fail to help. It can actively make things significantly worse.
Pathological demand avoidance vs oppositional defiant disorder comes up constantly in parenting forums, in school meetings, and in clinical offices, because both profiles involve a child or adult who refuses, resists, and pushes back against everyday demands and expectations. From the outside, the behavior can look the same. From the inside, the two are driven by completely different mechanisms, and that difference changes everything about what genuinely helps.
This post breaks down pathological demand avoidance vs oppositional defiant disorder clearly, explains what distinguishes them, and gives parents and adults a practical framework for understanding which one they might actually be dealing with.
Table of Contents
Pathological Demand Avoidance vs Oppositional Defiant Disorder: The Core Difference
What Is Pathological Demand Avoidance
What Is Oppositional Defiant Disorder
Pathological Demand Avoidance vs Oppositional Defiant Disorder: Side by Side
Why the Two Get Confused So Often
The Anxiety Question
How Each Profile Responds to Discipline
Can Someone Have Both
Getting an Accurate Assessment
What Actually Helps Each Profile
Final Thoughts
Pathological Demand Avoidance vs Oppositional Defiant Disorder
Pathological demand avoidance vs oppositional defiant disorder ultimately comes down to one core question: what is driving the resistance.
Oppositional defiant disorder is a behaviorally defined condition characterized by a persistent pattern of angry, defiant, and vindictive behavior directed at authority figures. The defiance is the central feature, and it typically responds, at least to some degree, to consistent behavioral management approaches.
Pathological demand avoidance, often discussed as a profile within autism, is driven by extreme anxiety related to a perceived loss of autonomy and control. The avoidance is not defiance for its own sake. It is a survival response triggered by demands themselves, regardless of how reasonable or appealing the demand actually is.
Pathological demand avoidance vs oppositional defiant disorder is therefore not really a question of which behaviors are present. Both can involve refusal, anger, and resistance. It is a question of what is underneath those behaviors, and that underlying mechanism determines which approaches will help and which will make things significantly worse.
What Is Pathological Demand Avoidance
Understanding pathological demand avoidance vs oppositional defiant disorder starts with a clear picture of what pathological demand avoidance actually is.
Pathological demand avoidance, often shortened to PDA, was first described by British psychologist Elizabeth Newson in the 1980s as a profile within the autism spectrum. It is characterized by an extreme and pervasive drive to avoid everyday demands and expectations, driven by anxiety about loss of autonomy rather than a simple desire to be defiant.
People with pathological demand avoidance experience ordinary requests, getting dressed, answering a question, sitting down to eat, as genuine threats to their sense of control. Their nervous system activates a fight, flight, or freeze response in reaction to demands, and from that activated state, compliance becomes neurologically very difficult rather than simply undesirable.
Pathological demand avoidance is not currently a formal diagnosis in the DSM-5, though awareness of the profile is growing steadily among clinicians who work with autistic individuals.
What Is Oppositional Defiant Disorder
The other half of pathological demand avoidance vs oppositional defiant disorder is ODD, a formally recognized diagnosis in the DSM-5.
Oppositional defiant disorder is defined by a pattern lasting at least six months of angry or irritable mood, argumentative or defiant behavior, and vindictiveness directed primarily at authority figures such as parents and teachers. To meet the diagnostic threshold, the behavior must occur with at least one person who is not a sibling and must be more frequent and intense than is typical for the person's developmental stage.
Common features of oppositional defiant disorder include frequent loss of temper, deliberately annoying others, blaming others for one's own mistakes, being easily annoyed by others, and a pattern of being spiteful or vindictive at least twice within a six month period.
ODD is generally understood as a behaviorally and emotionally driven condition, and it typically responds, with appropriate intervention, to structured behavioral approaches including consistent consequences, clear expectations, and positive reinforcement systems.

Comparing Pathological demand avoidance and oppositional defiant disorder
Pathological Demand Avoidance vs Oppositional Defiant Disorder: Side by Side
Putting pathological demand avoidance vs oppositional defiant disorder directly next to each other makes the distinction clearer:
Underlying driver: Pathological demand avoidance is driven by anxiety about loss of autonomy and control. Oppositional defiant disorder is driven by a pattern of angry, defiant, and vindictive behavior toward authority.
Target of the behavior: Pathological demand avoidance is triggered by demands themselves, regardless of who is making them or what the demand actually is. Oppositional defiant disorder is typically directed specifically at authority figures and tends to be more relationship-specific.
Response to a desirable demand: A person with pathological demand avoidance may avoid a demand even when the underlying activity is something they genuinely want to do, because the demand itself, not the activity, is the trigger. A person with oppositional defiant disorder is more likely to comply with demands around activities they want to do and resist demands around activities they do not want to do.
Response to choice and autonomy: Pathological demand avoidance significantly improves when autonomy and choice are genuinely increased. Oppositional defiant disorder does not respond to increased autonomy in the same predictable way and often requires consistent structure and boundaries instead.
Social presentation: Pathological demand avoidance frequently involves surface social skills that can appear sophisticated, including the use of social strategies to avoid demands. Oppositional defiant disorder typically does not involve this kind of social camouflaging.
Underlying condition: Pathological demand avoidance is understood as a profile within autism. Oppositional defiant disorder can occur independently or alongside other conditions including ADHD, anxiety disorders, and sometimes autism itself.
Why the Two Get Confused So Often
Pathological demand avoidance vs oppositional defiant disorder gets confused constantly, and there are specific reasons why.
Both profiles involve a child or adult refusing requests, becoming angry when pushed, and pushing back against authority. From a purely behavioral observation standpoint, without understanding what is driving the behavior, the two can look extremely similar in a single moment or even across several incidents.
Many clinicians, teachers, and parents were trained or grew up understanding defiance primarily through a behavioral lens, where resistance to authority is interpreted as a willful choice rather than as a potential symptom of underlying anxiety. This makes oppositional defiant disorder the more familiar, more readily reached-for explanation, even when pathological demand avoidance is actually the more accurate one.
Additionally, pathological demand avoidance is not in the DSM-5, which means clinicians working within strict diagnostic frameworks may default to oppositional defiant disorder simply because it is the available, billable diagnosis, even in cases where the underlying presentation more closely matches pathological demand avoidance.
The Anxiety Question
One of the most useful diagnostic questions in pathological demand avoidance vs oppositional defiant disorder is simply: where is the anxiety, and what is it about?
In pathological demand avoidance, anxiety is central and specific. It is anxiety about loss of control and autonomy, triggered consistently by demands of almost any kind. This anxiety is often visible even during refusal, manifesting as genuine distress rather than calculated defiance.
In oppositional defiant disorder, anxiety may or may not be present as a co-occurring condition, but it is not the defining driver of the oppositional behavior itself. The defiance in ODD is more closely tied to anger, frustration, and a pattern of conflict with authority rather than to an anxiety response specifically about demands and autonomy.
Asking what is actually happening internally in the moments before refusal, panic and overwhelm versus anger and a desire to assert control, often provides one of the clearest signals in distinguishing pathological demand avoidance vs oppositional defiant disorder.
How Each Profile Responds to Discipline
This is one of the most practically important parts of pathological demand avoidance vs oppositional defiant disorder, because the standard advice for ODD can significantly worsen pathological demand avoidance.
Oppositional defiant disorder generally responds, over time and with consistency, to structured behavioral approaches including clear consequences, reward systems, firm and predictable boundaries, and parent training programs designed specifically for ODD.
Pathological demand avoidance typically gets worse, not better, with these same approaches. Increased structure, increased consequences, and increased pressure all raise the demand load, which increases the anxiety driving the avoidance, which increases the avoidance itself. What helps with pathological demand avoidance instead is reducing the experience of external demand, increasing genuine autonomy and choice, and using indirect language rather than direct instruction.
This is exactly why getting pathological demand avoidance vs oppositional defiant disorder right matters so much in practice. Using the wrong framework does not just fail to help. It can create a worsening cycle that becomes increasingly difficult to interrupt.
If this feels personal, Sonia's coaching can help you build practical strategies for social and emotional challenges that fit you.
Can Someone Have Both
Pathological demand avoidance vs oppositional defiant disorder is not always a strict either-or question, and it is worth being honest about that.
It is possible for oppositional defiant disorder to be diagnosed alongside autism, including in individuals who also show pathological demand avoidance features. It is also possible for a child or adult who is actually experiencing pathological demand avoidance to be misdiagnosed with oppositional defiant disorder simply because that was the diagnostic framework available to the clinician at the time.
This is why getting a thorough, autism-informed assessment matters so much when pathological demand avoidance vs oppositional defiant disorder is genuinely unclear. A surface-level behavioral assessment alone is often not enough to distinguish the two accurately.
Getting an Accurate Assessment
Because pathological demand avoidance is not currently in the DSM-5, getting it properly recognized as part of the pathological demand avoidance vs oppositional defiant disorder distinction requires working with a clinician who has specific experience with the profile.
Useful steps include seeking assessment from a clinician with specific autism and PDA experience rather than a general behavioral evaluation alone, using the Extreme Demand Avoidance Questionnaire, a validated tool developed specifically to assess the PDA profile, documenting specific examples of avoidance across multiple settings including home, school, and community, and paying close attention to whether autonomy and choice genuinely reduce the avoidance, which is a strong indicator pointing toward PDA rather than ODD.
For a complete picture of what pathological demand avoidance involves and what genuinely helps, the full post on pathological demand avoidance in autism covers the profile in depth.
What Actually Helps Each Profile
Given everything above, pathological demand avoidance vs oppositional defiant disorder requires genuinely different support strategies.
For oppositional defiant disorder, what generally helps includes parent management training, consistent and predictable consequences, positive reinforcement for cooperative behavior, and family therapy approaches that address communication and conflict patterns within the family system.
For pathological demand avoidance, what generally helps includes reducing the overall demand load wherever possible, framing requests as genuine choices rather than instructions, using indirect and collaborative language, building trust and relationship as the foundation rather than compliance, and creating low-demand recovery periods when anxiety is high.
Getting pathological demand avoidance vs oppositional defiant disorder right is not just an academic exercise. It is the difference between a support plan that genuinely helps and one that actively makes things worse.
Final Thoughts
Pathological demand avoidance vs oppositional defiant disorder is a distinction that genuinely matters, not as an academic exercise but as a practical question that shapes whether the support a child or adult receives actually helps or actively makes things worse.
If the standard approaches to defiance are not working, or are making things significantly worse, pathological demand avoidance is worth seriously considering as the more accurate explanation. Getting the right framework, and the right support that follows from it, can change everything.
References:
Burns R. Is PDA in the DSM? What 'PDA-Style' Demand Avoidance Means [Internet]. ScienceWorks Behavioral Healthcare; 2025 Dec 17. Available from: https://www.scienceworkshealth.com/post/pda-not-in-dsm-what-clinicians-mean-by-pda-style-demand-avoidance
Burns R. PDA vs ODD: How Demand Avoidance Differs from Defiance [Internet]. ScienceWorks Behavioral Healthcare; 2025 Nov 18. Available from: https://www.scienceworkshealth.com/post/pda-anxiety-or-oppositional-making-sense-of-demand-avoidance
Baker S. Extreme Demand Avoidance Questionnaire – Adult (EDA-QA) [Internet]. NovoPsych; 2025 Dec 4. Available from: https://novopsych.com/assessments/autism/extreme-demand-avoidance-questionnaire-adult-eda-qa/
O'Nions E, Gould J, Christie P, Gillberg C, Viding E, Happé F. Identifying features of 'pathological demand avoidance' using the Diagnostic Interview for Social and Communication Disorders (DISCO). Eur Child Adolesc Psychiatry. 2015;25:407-419. Available from: https://doi.org/10.1007/s00787-015-0740-2

What Is Level 3 Autism? A Complete Guide for Parents and Families
What is level 3 autism is a question that often comes with real weight behind it, because Level 3 sits at the most complex end of the autism spectrum and the answer touches on some of the biggest, most life-shaping questions a parent or family member can ask. If you are here because your child, sibling, or loved one has just received this designation, or because you suspect it might apply, you deserve a clear, honest, and complete answer.
What is level 3 autism in the simplest terms is the official DSM-5 designation for autistic individuals who require very substantial support. It is the highest of the three official autism support levels, describing the most significant and pervasive impact on social communication and behavior that the diagnostic system currently recognizes.
This post answers what is level 3 autism in full, what it actually looks like in daily life, how it compares to Level 1 and Level 2, and what genuinely helps families and individuals navigating this end of the spectrum.
Table of Contents
What Is Level 3 Autism?
Where Level 3 Autism Sits on the Spectrum
Signs and Characteristics of Level 3 Autism
Communication and Level 3 Autism
Level 3 Autism vs Level 2 Autism
Level 3 Autism vs Level 1 Autism
How Level 3 Autism Is Diagnosed
What Daily Life Looks Like With Level 3 Autism
What Level 3 Autism Does Not Mean
What Support Actually Looks Like for Level 3 Autism
Final Thoughts
What Is Level 3 Autism?
What is level 3 autism according to the DSM-5? It is described as requiring very substantial support, the most significant of the three official levels. The manual defines it as severe deficits in verbal and nonverbal social communication skills that cause severe impairments in functioning, along with restricted, repetitive behaviors that markedly interfere with functioning across all areas of life.
What is level 3 autism in practical terms is a profile where support is not occasional or supplementary. It is constant, pervasive, and necessary across nearly every domain of daily living, including communication, self-care, safety, and community participation.
What is level 3 autism not is a measure of a person's worth, potential for connection, or capacity for a meaningful life. It is a description of current support needs as assessed in a specific clinical evaluation. It tells you how much support someone needs right now. It does not tell you who they are or what they are capable of experiencing, learning, or feeling.
Where Level 3 Autism Sits on the Spectrum
Understanding what is level 3 autism means seeing it clearly against the other two levels.
Level 1 autism involves support needs that a person can often manage with personal effort, without support being constantly present. Level 2 autism involves support needs that remain apparent and necessary even when support is actively provided, but that still allow for meaningful independence in some areas of life.
Level 3 autism involves support needs that are severe and pervasive enough that they affect functioning across nearly all domains, even when substantial, consistent support is already in place. What is level 3 autism, set against this scale, is the profile with the most significant and far-reaching impact on daily functioning that the current diagnostic system describes.
Signs and Characteristics of Level 3 Autism
What is level 3 autism actually looks like in practice involves a combination of communication, behavioral, and sensory characteristics that are significant and consistent across settings.
Social communication characteristics:
Very limited initiation of social interaction, often appearing to show minimal interest in social engagement as it is typically understood
Minimal response to social overtures from others, including from familiar caregivers
Severe difficulties with both verbal and nonverbal communication
Communication, when present, is often limited to expressing immediate needs rather than broader social or emotional exchange
Restricted and repetitive behavior characteristics:
Repetitive behaviors that are intense, frequent, and significantly interfere with functioning across multiple settings
Extreme distress in response to changes in routine or environment
Restricted interests or behaviors that dominate a significant portion of daily activity
Difficulty redirecting attention away from repetitive patterns even with active support
Sensory characteristics:
Significant sensory sensitivities that affect what environments and activities are tolerable
Strong reactions to sensory input that others may not perceive at all
Sensory needs that require ongoing, active accommodation rather than occasional adjustment
Daily functioning characteristics:
Significant support needs across most or all areas of daily living, including self-care tasks such as dressing, hygiene, and eating
Safety awareness that requires ongoing supervision and support
Higher rates of co-occurring conditions including epilepsy, gastrointestinal issues, and sleep disorders

Communication and Level 3 Autism
Communication is one of the most significant areas affected by what is level 3 autism, and it is also one of the areas where the right support makes the most measurable difference.
Many individuals with Level 3 autism have little to no functional spoken language. This does not mean they have nothing to communicate. It means spoken language is not a reliable channel for them to express their needs, preferences, and experiences.
Augmentative and Alternative Communication, known as AAC, is often transformative for individuals with Level 3 autism. This ranges from simple picture exchange systems to sophisticated speech generating devices, and finding the right communication channel is consistently one of the highest impact interventions available.
It is worth being direct about something important here: a person with Level 3 autism who cannot speak is not a person without thoughts, preferences, or an inner life. They are a person whose primary communication channel has not yet been found or fully supported. The research on AAC consistently shows that many nonverbal autistic individuals have far more to communicate than their spoken output suggests once the right tool is in place.
Level 3 Autism vs Level 2 Autism
Comparing what is level 3 autism against what is level 2 autism helps clarify exactly where the line sits between them.
Level 2 autism involves social communication deficits that remain apparent even with support, but the person often retains functional spoken language and can manage some independence in daily living with consistent structural support. Level 3 autism involves more severe deficits that cause significant impairment even with very substantial support actively in place, and functional spoken language is frequently absent or extremely limited.
Repetitive behaviors at Level 2 interfere with functioning across multiple settings but are often manageable with redirection and support. At Level 3, these behaviors are more intense and markedly interfere with functioning even when active support is provided.
Daily living independence is more achievable at Level 2 in many domains. At Level 3, support needs typically extend across nearly all areas of daily living, including self-care and safety.
For a complete look at what Level 2 autism involves specifically, the post on what is level 2 autism covers that middle point on the spectrum in full detail.

Level 3 Autism vs Level 1 Autism
Comparing what is level 3 autism against what is level 1 autism shows the full range the diagnostic system is trying to capture under a single spectrum.
Level 1 autism, sometimes informally called high functioning autism, involves support needs that a person can often manage independently, with social communication challenges that are noticeable but generally compatible with functioning in most everyday settings without support being constantly present.
Level 3 autism sits at the opposite end, with support needs that are constant, pervasive, and necessary across nearly every area of daily life, even when substantial support is already in place. Aside these, Dropped in a Maze provides a clear picture on how to navigate autism.
The distance between these two ends of the spectrum is part of why autism is described as a spectrum rather than a single condition with one presentation. Two people can both carry an autism diagnosis and have profiles, support needs, and daily experiences that look almost entirely different from one another. For a closer look at the other end of this range, the post on what is level 1 autism covers that presentation in depth.
How Level 3 Autism Is Diagnosed
What is level 3 autism in terms of the actual diagnostic process follows the same general framework used across the spectrum, though the evaluation often happens earlier in life because the signs tend to be more pronounced and visible from a younger age.
A comprehensive evaluation typically includes a detailed developmental history from parents or caregivers, direct behavioral observation using tools such as the ADOS-2, cognitive and language assessment adapted for the individual's communication level, and input from other professionals including speech therapists and occupational therapists who know the child or adult well.
For a full walkthrough of the entire testing and diagnostic process from first screening through to full evaluation, the post on how to test for autism covers exactly what families can expect at every stage.
What Daily Life Looks Like With Level 3 Autism
What is level 3 autism in lived, daily terms varies depending on the individual, but it generally involves a level of structure, support, and consistency that shapes most of the day.
Daily routines are often highly structured because predictability significantly reduces distress and supports functioning. Communication happens through whatever channel works best for that individual, whether AAC devices, gestures, behavior, or limited functional speech. Sensory environments are actively managed, with lighting, sound, and textures considered and adjusted wherever possible. Safety supervision is ongoing rather than occasional, particularly for individuals who may not reliably understand environmental risks.
None of this means daily life with Level 3 autism is without joy, connection, or genuine quality of life. Many individuals with Level 3 autism experience real happiness, form meaningful bonds with the people who know how to connect with them, and respond strongly to music, movement, sensory play, and the presence of people who make them feel safe.
Level 3 Autism
What Level 3 Autism Does Not Mean
This matters as much as anything else in this post, because some of the most harmful assumptions about Level 3 autism come from what people wrongly believe the label implies.
What is level 3 autism does not mean the person has no inner life, no preferences, and no capacity for growth. It does not mean communication is impossible, only that spoken language may not be the right channel. It does not mean the person cannot learn or make meaningful progress with the right support over time. It does not mean their life has less value than the life of someone with Level 1 autism. It does not mean families should lower their hopes for connection and quality of life.
The person is always there. What changes with the right support is how clearly the people around them can see and understand who that person actually is.
What Support Actually Looks Like for Level 3 Autism
Support for what is level 3 autism needs to be comprehensive, consistent, and genuinely tailored to the individual, drawing on several areas working together.
Communication support through AAC evaluation and implementation is consistently one of the highest impact interventions. Educational support under an IEP that addresses communication, behavioral, and daily living goals specifically is essential. Behavioral support that is positive and function-based, focused on understanding what a behavior is communicating rather than simply suppressing it, produces far better outcomes than punitive approaches. Medical management addressing the higher rates of epilepsy, gastrointestinal issues, and sleep disorders associated with Level 3 autism is an important and often overlooked part of comprehensive care.
Ready to navigate this with support? Sonia, a licensed psychotherapist provides Adult Coaching Services
Final Thoughts
What is level 3 autism is, at its core, a description of the most significant and pervasive support needs the current diagnostic system recognizes. It is not a description of a person's worth, their capacity for connection, or the ceiling on their growth.
The families and individuals navigating Level 3 autism deserve fully resourced, genuinely informed, deeply compassionate support, and that support, when it arrives in the right form at the right time, makes a real and lasting difference to quality of life for everyone involved.
References:
Iacono T, Trembath D, Erickson S. The role of augmentative and alternative communication for children with autism: current status and future trends. Neuropsychiatr Dis Treat. 2016;12:2349-2361. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5036660/
Lin W, Chan YH, Kiing JSH, Lim TSH, Chong SC, Kang YQ, Aishworiya R, Mulay KV, Tan MY. Restricted and repetitive behaviors and association with cognition and adaptive functioning in children with autism spectrum disorder in Singapore. Front Psychiatry. 2023;14:1249071. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10687550/
American Speech-Language-Hearing Association. Augmentative and Alternative Communication in Early Intervention [Internet]. Available from: https://www.asha.org/practice/early-intervention-provider-support/augmentative-and-alternative-communication-in-early-intervention/
Maddox BB, Brodkin ES, Calkins ME, Shea K, Mullan K, Hostager J, Mandell DS, Miller JS. The accuracy of the ADOS-2 in identifying autism among adults with complex psychiatric conditions. J Autism Dev Disord. 2017;47(9):2703-2709. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5813679/

What Is Level 2 Autism? A Complete Guide for Adults
What is level 2 autism is a question that often comes up after someone has already read about Level 1 and felt like the description did not quite fit, like their experience involves more visible struggle, more daily friction, and more support than what is typically described as the lighter end of the spectrum. If that is where you are right now, you are asking exactly the right question.
What is level 2 autism in the simplest terms is the official DSM-5 designation for autistic individuals who require substantial support in social communication and who show restricted or repetitive behaviors that interfere with functioning across multiple settings, even when some support is already in place. It sits in the middle of the three official autism levels, more visible and more demanding than Level 1, less pervasive than Level 3.
This post answers what is level 2 autism in full, what it actually looks and feels like for adults living with it, how it compares to Level 1 and Level 3, and what genuinely helps.
Table of Contents
What Is Level 2 Autism?
Where Level 2 Autism Sits on the Spectrum
Signs of Level 2 Autism in Adults
Level 2 Autism vs Level 1 Autism
Level 2 Autism vs Level 3 Autism
Why Level 2 Autism Is Often Missed or Misread in Adults
Getting Assessed for Level 2 Autism as an Adult
What Support Actually Looks Like for Level 2 Autism
Building a Life That Works With Level 2 Autism
FAQs
Final Thoughts
What Is Level 2 Autism?
What is level 2 autism according to the DSM-5? It is the diagnostic category for autistic individuals who require substantial support. The manual describes this as marked deficits in verbal and nonverbal social communication skills, social impairments that are apparent even with support in place, and restricted, repetitive behaviors that interfere with functioning in a variety of contexts.
What is level 2 autism in practical terms is a profile that sits clearly between Level 1, which involves less visible support needs, and Level 3, which involves very substantial support needs across nearly all areas of life. Level 2 is the middle ground, and it is a middle ground that often gets less attention in public conversation than either end of the spectrum, despite affecting a significant number of autistic adults.
What is level 2 autism not is a fixed, unchanging category that determines everything about a person's potential. It describes support needs at a point in time, assessed through specific clinical observation, not a ceiling on what someone can learn, achieve, or become with the right environment around them.
Where Level 2 Autism Sits on the Spectrum
Understanding what is level 2 autism requires seeing it in context against the other two levels.
Level 1 autism involves social communication difficulties that are noticeable but that allow the person to function largely independently in most settings without support, alongside restricted or repetitive behaviors that the person can usually manage with effort.
Level 2 autism involves social communication deficits that remain apparent even when support is actively provided, meaning the person needs that support to be present and ongoing rather than occasional, alongside restricted or repetitive behaviors that interfere with functioning across multiple settings and that are more difficult to redirect or manage than at Level 1.
Level 3 autism involves severe social communication deficits that cause significant impairment even with substantial support in place, alongside repetitive behaviors that markedly interfere with functioning in essentially every domain of life.
What is level 2 autism, set against this scale, is a profile where the support is not optional or occasional. It is genuinely needed, genuinely ongoing, and genuinely makes a difference in how well the person is able to function day to day.
What to know about level 2 Autism
Signs of Level 2 Autism in Adults
What is level 2 autism in adults looks different from a childhood checklist, and recognizing it in your own adult life requires looking at how these traits show up across work, relationships, and daily independence.
Social communication signs:
Communication that others frequently describe as difficult to follow, overly literal, or hard to engage with in typical back and forth conversation, even when support and patience are offered by the other person
Significant difficulty initiating social interaction without a clear script or specific purpose
A need for very explicit, very direct communication from others, with ambiguity or implied meaning causing genuine confusion rather than mild friction
Social interactions that remain effortful and draining even after years of practice and even in relationships with people who are familiar and supportive
Restricted and repetitive pattern signs:
Repetitive behaviors or routines that are difficult to interrupt or redirect, even by people close to you
Significant distress, not just mild discomfort, when routines or environments change unexpectedly
Restricted interests that take up a substantial portion of daily life and that are hard to set aside even when other demands are present
Sensory responses that are intense enough to regularly affect what environments and activities are realistically possible for you
Daily functioning signs:
Needing consistent, ongoing support from a partner, family member, or support worker to manage tasks that most adults handle independently, such as scheduling, finances, or household management
Difficulty maintaining employment without specific accommodations and ongoing support in place
A pattern of needing more structure and more external scaffolding than peers in order to get through an ordinary day
If a significant number of these genuinely describe your daily life, what is level 2 autism may be a far more accurate and useful framework for understanding yourself than the less intensive descriptions you may have read elsewhere.
Level 2 Autism vs Level 1 Autism
One of the most useful ways to understand what is level 2 autism is to directly compare it against what is level 1 autism, since many adults read about one before recognizing themselves more clearly in the other.
The core difference is the visibility and ongoing necessity of support. A person with Level 1 autism can generally function without support present in the moment, even if doing so is exhausting and effortful. A person with Level 2 autism needs the support to actually be there, consistently, for daily functioning to genuinely work.
Social communication difficulties are noticeable in both levels, but at Level 1 they tend to be manageable with personal effort and masking, while at Level 2 they remain apparent and disruptive even when support and accommodation are actively in place.
Restricted and repetitive behaviors at Level 1 typically affect functioning in a more limited way, often in just one or two specific contexts. At Level 2, these behaviors interfere across multiple settings and are noticeably harder to redirect or interrupt.
For a deeper look specifically at what is level 1 autism and how it presents in adults, including the specific masking patterns and missed diagnosis issues that come with it, the dedicated post on what is level 1 autism covers that end of the spectrum in full.

Comparing Level 2 Autism vs Level 3 Autism
Level 2 Autism vs Level 3 Autism
It is equally useful to understand where what is level 2 autism stops and Level 3 begins, since the line between them is not always obvious from a self-assessment alone.
Level 3 autism involves severe deficits in social communication that cause very significant impairment even with very substantial support in place. Level 2 involves deficits that are serious and require real support, but the impairment, even without that support fully optimized, is generally less severe than at Level 3.
Level 3 typically involves very limited functional verbal communication or none at all. Level 2 frequently involves functional spoken language, even if that language is unusual in structure, tone, or use.
Level 3 generally requires support across nearly every domain of daily living, often including self-care. Level 2 requires substantial support in specific domains, particularly social communication and behavioral regulation, but often allows more independence in other areas of daily life.
For a full comparison of how profound autism specifically relates to these official levels, the post on profound autism vs autism level 3 is worth reading if you suspect your needs may extend beyond what is described here.
Why Level 2 Autism Is Often Missed or Misread in Adults
What is level 2 autism, despite being more visible than Level 1, is still frequently missed, delayed, or misread in adults, for reasons that are worth understanding.
It gets misread as something else entirely: Adults with undiagnosed Level 2 autism are frequently given other labels first, including intellectual disability when the issue is actually communication style rather than cognitive ability, personality disorders when the issue is actually autistic rigidity and social difference, or simply being labeled as difficult, demanding, or high maintenance by people who do not understand what they are actually observing.
Adult diagnostic pathways are less developed for this level: Much of adult autism diagnosis has historically focused on identifying Level 1 presentations in people who mask well. Diagnostic pathways and public awareness for adult Level 2 presentations are less developed, meaning adults with this profile may struggle to find evaluators who recognize their presentation accurately.
The support need gets attributed to other causes: When an adult clearly needs substantial ongoing support, that need is sometimes attributed to anxiety, low motivation, or poor life skills rather than being recognized as a feature of an underlying autism profile that has simply never been formally assessed.
Getting Assessed for Level 2 Autism as an Adult
If what is level 2 autism is sounding like an accurate description of your own life, formal assessment can provide genuine clarity and can open access to support that has previously been unavailable without a diagnosis.
Adult assessment for Level 2 autism typically involves the same core tools used across the spectrum, including the ADOS-2, a detailed developmental history, and direct clinical observation, but ideally conducted by an evaluator with specific experience recognizing presentations beyond the more commonly discussed Level 1 profile. Also, there are books that help. Dropped by a Maze is a recommended book to read to help through diagnosis.
For a complete walkthrough of the entire testing and diagnostic process, from initial screening through full evaluation, the post on how to test for autism covers exactly what to expect at every stage.
Building a Life That Works With Level 2 Autism
What is level 2 autism, ultimately, is a profile that genuinely benefits from intentional, well-supported life design rather than an expectation that the person will simply adapt to a world that was not built with them in mind.
This is exactly the work Sonia's coaching focuses on. Socio-emotional coaching helps adults with Level 2 autism build practical, personalized strategies for navigating relationships, work, and daily structure in ways that genuinely fit their actual needs rather than forcing them into a one-size-fits-all approach to independence.
Self-esteem coaching addresses the accumulated impact of years spent being seen as too much, too difficult, or too demanding, helping rebuild a sense of identity grounded in accurate self-understanding rather than years of feeling like a burden for needing real support.
What Support Actually Looks Like for Level 2 Autism
Support for what is level 2 autism in adulthood needs to be genuinely substantial and genuinely ongoing, not occasional or symbolic, in order to make a real difference.
Useful forms of support include consistent, structured routines built collaboratively rather than imposed, clear and explicit communication from the people around you rather than reliance on implied meaning, sensory accommodations in the home and work environment, and coaching or therapy specifically focused on building practical life skills and self-advocacy rather than only addressing secondary anxiety or depression.
Workplace support, where employment is part of the picture, often needs to include written instructions, predictable schedules, a clearly defined role with explicit expectations, and a manager or colleague willing to communicate directly rather than relying on social inference.
Final Thoughts
What is level 2 autism is, at its core, a profile that requires real, ongoing, substantial support to allow for genuine daily functioning, and that support need is not a sign of failure or inadequacy. It is simply what this particular neurology requires in order to thrive.
If what is level 2 autism has started to sound like an accurate description of your own experience, pursuing formal assessment and seeking out support that is built around your actual needs, rather than a watered-down version designed for a different presentation entirely, is a meaningful and worthwhile next step.
References:
Autism Speaks. ASD levels of severity [Internet]. Available from: https://www.autismspeaks.org/levels-of-autism
National Academies of Sciences, Engineering, and Medicine. Autism: Prevalence, Diagnosis, and Interventions. In: The Comprehensive Autism Care Demonstration: Solutions for Military Families. Washington (DC): National Academies Press (US); 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK619283/
What Is Level 1 Autism? A Complete Guide for Adults
What is level 1 autism is a question a lot of adults end up searching late at night, often after a conversation that did not quite land the way it should have, or after watching a video about autism and feeling an uncomfortable jolt of recognition. If you are here because you suspect level 1 autism might explain something about your own life, you are not overreacting. You are paying attention.
What is level 1 autism in the simplest possible terms is the official diagnostic category for autistic individuals who need some support but who function independently in many areas of daily life. It is the part of the spectrum that is hardest to spot from the outside and hardest to live with quietly on the inside, because the struggle is real even when it is invisible to everyone around you.
This post answers what is level 1 autism in full, what it actually feels like to live with from the inside, how it differs from other autism levels, and what comes next if you recognize yourself in what you read.
Table of Contents
What Is Level 1 Autism?
Where Level 1 Autism Fits on the Spectrum
Signs of Level 1 Autism in Adults
What Level 1 Autism Feels Like From the Inside
Why Level 1 Autism Is So Often Missed in Adults
Level 1 Autism and Masking
Level 1 Autism and Mental Health
Getting Assessed for Level 1 Autism as an Adult
What Support Actually Looks Like for Level 1 Autism
Life After Recognizing Level 1 Autism in Yourself
FAQs
Final Thoughts

What Is Level 1 Autism?
What is level 1 autism according to the DSM-5? It is the diagnostic label given to autistic individuals who, in the language of the manual, require support. This is the lowest support level on the official three-tier system, sitting below Level 2, which requires substantial support, and Level 3, which requires very substantial support.
What is level 1 autism in practical terms is autism that allows a person to live, work, and function across most everyday settings without needing constant external support, while still experiencing real and sometimes significant challenges in social communication and in managing restricted or repetitive patterns of behavior.
What is level 1 autism not is autism that is mild, easy, or somehow less real than the rest of the spectrum. The word level here describes visible support needs as assessed in a specific evaluation, not the internal effort, exhaustion, or struggle a person experiences day to day. Many people with what is clinically labeled level 1 autism describe their daily life as anything but easy.
For a complete breakdown of all three autism levels and how they compare to one another, the post on what are the levels of autism: a guide for parents covers Level 1, Level 2, and Level 3 side by side in detail.
Where Level 1 Autism Fits on the Spectrum
Understanding what is level 1 autism requires understanding where it sits relative to the other two levels.
Level 1 autism involves noticeable difficulties with social communication that are not severe enough to prevent functioning without support in most settings, alongside restricted or repetitive behaviors that cause some interference with functioning in one or more contexts but that the person can often manage with effort.
Level 2 autism involves more substantial social communication challenges that are apparent even with support in place, and restricted or repetitive behaviors that interfere with functioning across multiple contexts and are harder to redirect.
Level 3 autism involves severe deficits in social communication that cause significant impairment even with support, alongside restricted or repetitive behaviors that markedly interfere with functioning across all areas of life.
What is level 1 autism, placed against this scale, is the presentation that looks the most capable from the outside and is therefore the one most likely to have its real struggles dismissed, minimized, or simply not believed.

How Autism Affects
Signs of Level 1 Autism in Adults
What is level 1 autism in adults looks different from the textbook descriptions that were largely built around observing children. Here is what it commonly looks like when it shows up in grown adults navigating careers, relationships, and independent life.
Social communication signs:
Difficulty with the unwritten rules of conversation including knowing when to speak, when to stop, and how to read when someone has lost interest
A tendency toward very literal interpretation of language, missing sarcasm, idioms, or implied meaning until it is explained directly
Genuine desire for connection paired with exhaustion after socializing, even socializing that went well
Difficulty maintaining friendships over time, not from lack of caring but from struggling with the ongoing maintenance that relationships require
Being told you come across as blunt, intense, or too direct when you did not intend to
Restricted and repetitive pattern signs:
One or more deep, narrow interests that you could talk about for hours given the chance
Strong need for routine and predictability, with real distress when plans change unexpectedly
Repetitive movements or habits, sometimes subtle, such as foot tapping, hair twirling, or specific verbal phrases you repeat under stress
Discomfort with open-ended or ambiguous situations that lack clear structure
Sensory signs:
Strong reactions to specific sounds, lights, textures, or smells that other people do not seem to notice at all
Needing to retreat and decompress after busy or loud environments
Preference for specific clothing textures or an inability to tolerate certain fabrics, tags, or seams
If several of these genuinely resonate, Sonia's coaching can help you build practical strategies for social and emotional challenges that fit you.
What Level 1 Autism Feels Like From the Inside
What is level 1 autism on paper and what level 1 autism feels like in a person's actual daily life are two very different things, and the gap between them is exactly why so many adults go undiagnosed for decades.
From the inside, level 1 autism often feels like running a constant background process that other people do not seem to be running. Every social interaction involves a layer of conscious calculation: what is the right facial expression here, how long should eye contact last, is this the moment to speak or stay quiet, did that comment mean what it sounded like or something else entirely.
It often feels like exhaustion that does not match the apparent size of the event that caused it. A birthday party, a work meeting, a casual coffee with a friend, things that look ordinary from the outside, can leave a person with level 1 autism needing hours or even days to recover.
It often feels like being told you are too sensitive, too rigid, too intense, or too much, by people who have no idea that what they are describing has a name and a reason behind it. To better understand this, Dropped by Maze explains this from a lived experience of Sonia Chand.
What is level 1 autism, lived rather than studied, is the experience of working significantly harder than most people around you just to arrive at outcomes that look, from the outside, ordinary and unremarkable.

What to know about Level 1 Autism
Why Level 1 Autism Is So Often Missed in Adults
What is level 1 autism, more than anything else, is the presentation most likely to be missed entirely, and there are specific reasons why.
Compensation and intelligence: Many adults with level 1 autism are highly intelligent and have spent years building sophisticated, often exhausting, workarounds for the things that do not come naturally. The compensation can be so effective that nobody, including the person themselves, realizes anything different is going on underneath it.
The wrong comparison point: Most people's mental image of autism comes from more visible presentations, often from childhood. An adult who holds a job, lives independently, and maintains some relationships does not match that image, so what is level 1 autism gets overlooked by professionals and loved ones alike.
Misdiagnosis along the way: Many adults with level 1 autism spent years collecting other diagnoses first, anxiety disorder, depression, social anxiety disorder, or even personality disorders, because those were the labels available to professionals who were not looking specifically for autism.
Gender bias in research and diagnosis: Women and people socialized as women are especially likely to have level 1 autism missed because diagnostic criteria were largely developed by observing boys, and because girls and women tend to mask more effectively from a young age.
Level 1 Autism and Masking
Masking is one of the central features of what is level 1 autism in adulthood, and it deserves its own real attention here.
Masking is the conscious or semi-conscious suppression of natural autistic traits in order to appear more neurotypical. For adults with level 1 autism, masking often becomes so automatic and so deeply practiced that it stops feeling like a performance and starts feeling like simply who they are, until exhaustion, burnout, or a major life change forces the mask to slip and the underlying reality becomes visible again.
Common masking behaviors in level 1 autism include forcing eye contact that feels physically uncomfortable, rehearsing conversations in advance, mimicking the tone and body language of people around you, and suppressing stimming behaviors in public only to release them once alone.
The cost of sustained masking is significant. It is strongly associated with anxiety, depression, and a specific kind of exhaustion known as autistic burnout, which can present as a sudden and frightening collapse in someone who appeared, to everyone around them, to be managing just fine.
Level 1 Autism and Mental Health
What is level 1 autism cannot be fully understood without understanding its close relationship with mental health, because the two are deeply intertwined for most adults living with this profile.
Research consistently shows elevated rates of anxiety and depression among autistic adults, and level 1 autism specifically carries a particular mental health burden because the demand to mask and to function at a neurotypical standard is highest precisely in this group. The very thing that makes level 1 autism less visible, the apparent capability, is also what denies many adults the recognition and support that would meaningfully reduce their mental health risk.
Many adults discovering what is level 1 autism for the first time describe genuine relief at finally understanding the root cause of years of anxiety or low mood that talk therapy alone never fully resolved, because the therapy was treating symptoms without addressing the underlying autistic experience driving them.
Getting Assessed for Level 1 Autism as an Adult
If what is level 1 autism has started to feel like it might be describing you specifically, formal assessment is available and increasingly accessible.
Adult autism assessment typically involves a detailed developmental history interview, standardized tools adapted for adults including the ADOS-2 Module 4, self-report questionnaires such as the Autism Spectrum Quotient, and a comprehensive clinical interview that explores both childhood history and current functioning.
Finding an assessor with specific experience in adult autism, and ideally specific experience with level 1 presentations and with women and people who mask effectively, makes a significant difference in the quality and accuracy of the assessment. For a full walkthrough of the entire testing process from screening through to diagnosis, the post on how to test for autism covers every stage in detail, including what to expect at each step.
Socio-emotional coaching helps with the very practical next step: learning how to navigate relationships, work, and daily life in ways that genuinely work with your level 1 autism rather than constantly fighting against it.
Book a socio-emotional coaching session with Sonia here and start building strategies that actually fit how your brain works.
What Support Actually Looks Like for Level 1 Autism
Support for what is level 1 autism in adulthood looks very different from support designed for children, and it is worth knowing what is genuinely available and helpful.
Useful forms of support include therapy or coaching with a practitioner who understands autism specifically rather than treating only the secondary anxiety or depression, workplace accommodations such as written instructions, flexibility around sensory environment, and clear expectations, structured routines that reduce daily decision fatigue, and connection with other late-identified autistic adults who understand the experience without needing it explained.
What tends not to help, and can actively cause harm, is any approach focused on making someone appear more neurotypical rather than helping them understand and work with their own neurology. The goal of good support for level 1 autism is never to eliminate the autism. It is to reduce the exhausting compensation and replace it with genuine understanding and accommodation.
Life After Recognizing Level 1 Autism in Yourself
Recognizing what is level 1 autism in your own life, whether through formal diagnosis or simply through deep self-recognition, often marks a genuine turning point, and it is worth being honest that the period right after this recognition can be emotionally complex.
There is frequently grief, for the years spent not understanding yourself, for the relationships that struggled under the weight of unexplained differences, for the energy spent compensating for something that had a name all along. There is also, very often, real relief, the kind that comes from finally having language for a lifetime of experiences that never quite made sense before.
This is exactly the territory where Sonia's coaching work becomes most valuable. Self-esteem coaching helps adults who are newly understanding their own level 1 autism rebuild a sense of identity that is not built on years of masking and self-criticism, but on an accurate and compassionate understanding of who they actually are.
Book a self-esteem coaching session with Sonia here and start building a sense of self that does not depend on the mask anymore.
FAQs
Is level 1 autism the same as high functioning autism?
The terms overlap significantly. High functioning autism is an informal term while Level 1 is the official diagnostic designation.
Can adults be diagnosed with level 1 autism?
Yes. Adult autism assessment is increasingly available and many adults are diagnosed with level 1 autism for the first time later in life.
Is level 1 autism the same as Asperger Syndrome?
They describe largely the same population. Asperger Syndrome was discontinued as a separate diagnosis in 2013 and folded into Level 1 autism under the DSM-5.
Why is level 1 autism so often missed in adults?
Effective masking, high intelligence, compensation strategies, and gender bias in diagnostic criteria all contribute to level 1 autism being frequently overlooked.
Does level 1 autism require support?
Yes. The word level 1 specifically means requiring support, just less visible or intensive support than Level 2 or Level 3.
What is the difference between level 1 and level 2 autism?
Level 2 involves more substantial social communication challenges and more pronounced repetitive behaviors that interfere with functioning across more settings than Level 1.
Final Thoughts
What is level 1 autism is ultimately a question with a fairly simple clinical answer and a far more complicated lived answer. Clinically, it describes autistic individuals who need support but who manage independently across many areas of daily life. In real life, it describes years of quiet exhaustion, of masking that nobody saw, of working twice as hard for outcomes that looked effortless from the outside.
If what is level 1 autism has started to sound like your own story, that recognition is worth taking seriously. Whether you pursue formal assessment, seek coaching support, or simply start reading and learning more, the clarity that comes from understanding your own neurology accurately is almost always better than continuing to carry an unexplained weight alone.
References:
Cleveland Clinic. Autism [Internet]. Available from: https://my.clevelandclinic.org/health/articles/autism
NovoPsych. Autism Spectrum Quotient (AQ) [Internet]. https://novopsych.com/assessments/diagnosis/autism-spectrum-quotient/
Evans JA, Krumrei-Mancuso EJ, Rouse SV. What You Are Hiding Could Be Hurting You: Autistic Masking in Relation to Mental Health, Interpersonal Trauma, Authenticity, and Self-Esteem. Autism Adulthood. 2024;6(2):229-240. https://pmc.ncbi.nlm.nih.gov/articles/PMC11317797/
Al Raish SM, Shokr MM, Eladawy RM, Azar YO. Depression in Autism Spectrum Disorder: Neurobiological Convergence and Emerging Therapeutic Strategies. Biology. 2026;15(10):745. https://doi.org/10.3390/biology15100745
Hus V, Lord C. The Autism Diagnostic Observation Schedule, Module 4: Revised Algorithm and Standardized Severity Scores. J Autism Dev Disord. 2014;44(8):1996-2012. https://pmc.ncbi.nlm.nih.gov/articles/PMC4104252/

If Autism Runs in Your Family: What You Need to Know
If autism runs in your family, you have probably already started asking yourself questions that feel hard to say out loud. Will my next child be autistic too? Does this mean I am autistic and never knew it? What does it mean for my nieces, my nephews, my grandchildren someday? If autism runs in your family, those questions are not anxious overthinking. They are reasonable questions with real, research-backed answers.
This post is for anyone who has looked around their family tree and started noticing a pattern. A sibling who was diagnosed. A cousin who was always a bit different. A parent who, looking back, almost certainly was on the spectrum and never knew it. If autism runs in your family, understanding what that actually means, genetically and practically, can replace anxious guessing with real clarity.
Table of Contents
If Autism Runs in Your Family: What You Need to Know
What the Genetics Actually Say
What Are the Actual Odds
Recognizing Autism Across Generations
If Autism Runs in Your Family and You Are Planning a Family
If Autism Runs in Your Family and You Suspect It Is You
What to Watch for in Your Children Early
Talking to Family Members About a Possible Pattern
What a Family History of Autism Does Not Mean
FAQs
Final Thoughts
If Autism Runs in Your Family: What You Need to Know
If autism runs in your family, the first thing worth knowing is that you are far from alone in noticing this. Autism is one of the most heritable neurodevelopmental conditions known to science, and family clustering of autism traits is a well-documented and well-researched phenomenon, not a coincidence or a pattern you are imagining.
If autism runs in your family, it usually shows up in one of a few recognizable ways. Sometimes it is a sibling pattern, where one child is diagnosed and a younger or older sibling is later identified as autistic too. Sometimes it is a generational pattern, where a parent recognizes their own traits clearly for the first time only after their child's diagnosis. And sometimes it is a wider pattern across cousins, aunts, uncles, and grandparents that becomes visible only once someone starts actively looking for it.
Whatever shape it takes in your specific family, if autism runs in your family it means there is a genuine genetic and neurological thread running through your relatives, and understanding that thread helps you make better decisions, ask better questions, and worry less about the unknown.

What the Genetics Actually Say
What the Genetics Actually Say
The scientific research on autism heritability is some of the most robust in all of neurodevelopmental research, and it consistently points to one clear conclusion: genetics play the dominant role in autism risk.
Twin studies, which are considered the gold standard for understanding the genetic contribution to any condition, have found that when one identical twin is autistic, the other twin has a significantly elevated chance of also being autistic, far higher than the rate seen in non-identical twins or in the general population. Current estimates suggest that genetic factors account for approximately 80 percent of autism risk.
What makes autism genetics complex is that there is no single autism gene. Instead, researchers have identified hundreds of genetic variants that each contribute a small amount of risk. Some of these variants are inherited from parents. Others arise spontaneously as new mutations in the affected individual. Most cases of autism likely involve a combination of many inherited common variants interacting with each other, rather than one single inherited mutation causing the condition outright.
This is part of why if autism runs in your family, the pattern is not always neat or predictable. You might have one autistic child and one who shows no autistic traits at all, even though both share the same parents and largely the same genetic background. The combination of variants each child inherits is different enough to produce very different outcomes.
What Are the Actual Odds
If autism runs in your family, you are likely wondering about actual numbers rather than general statements about heritability. Here is what the research shows.
If you already have one autistic child: Research suggests that the chance of a younger sibling also being autistic is significantly elevated compared to the general population, with studies estimating recurrence rates between 10 and 20 percent depending on the specific study and the sex of the children involved. Families with two or more autistic children have an even higher chance of additional children being autistic.
If you are autistic yourself: Children of autistic parents have a notably higher chance of being autistic themselves compared to children of non-autistic parents, reflecting the strong heritable component of the condition.
If a sibling, cousin, or more distant relative is autistic: The closer the genetic relationship, the higher the elevated risk. A sibling relationship carries more weight than a cousin relationship, which carries more weight than a more distant relative.
Sex differences matter: Research consistently shows that male children have a higher likelihood of being diagnosed with autism than female children, even within the same family, which is part of why if autism runs in your family the pattern can look different depending on which children are boys and which are girls.
These numbers are population averages and not predictions for any individual family. They are useful for understanding general risk levels, not for telling you with certainty what will happen with your own children.
For families who are in the process of getting a formal answer for a specific child, understanding the testing and diagnostic process is the next practical step. The post on how to test for autism walks through exactly how that process works from first screening to full diagnosis.

How to recognize Autism across generations
Recognizing Autism Across Generations
If autism runs in your family, one of the most common experiences is realizing that the pattern did not start with your child. It started further back, with relatives who were never diagnosed because the diagnostic criteria, the cultural awareness, and the available language for autism simply did not exist in the way it does now.
Older generations often described autistic relatives using language that had nothing to do with autism at all. He was just quirky. She was always in her own world. He never talked much but he was brilliant with numbers. She was painfully shy but knew everything about birds. These descriptions, looked at through a modern lens, often describe autistic traits that went entirely unrecognized and unsupported throughout that person's life.
If autism runs in your family across multiple generations, it is worth having open conversations with older relatives, where possible and appropriate, about what their own childhood and adulthood actually felt like. Many adults in their fifties, sixties, and seventies are recognizing themselves as autistic for the first time only after a grandchild's diagnosis prompts them to look honestly at their own life.
This generational recognition is not about assigning a label retroactively for its own sake. It is about understanding the fuller picture of what runs in your family and using that understanding to support every generation more effectively, including the ones who are still here to benefit from it.
If you’re ready to stop figuring this out alone? Sonia works with individuals and families navigating neurodivergent journeys through personalized one-on-one coaching sessions. Spots are limited. Book your session here.
If Autism Runs in Your Family and You Are Planning a Family
If autism runs in your family and you are currently planning to have children or to have more children, the genetic information above is likely sitting somewhere in the back of your mind as you make that decision.
It is worth being honest about a few things here. First, there is currently no reliable prenatal genetic test that can predict whether a child will be autistic. Autism involves too many genetic variants interacting in too many combinations for any single test to provide a clear answer. Anyone offering you a definitive predictive test for autism risk in an unborn child is overstating what the science can currently do.
Second, the elevated statistical risk that comes with having autism in your family is real, but it describes a probability, not a certainty. The vast majority of children born into families with a strong autism history are not autistic. And many children who are autistic go on to live full, connected, meaningful lives with the right support.
Third, if autism runs in your family, the most useful thing you can do while planning a family is not to try to predict or prevent an autism diagnosis. It is to prepare yourself with knowledge, build relationships with pediatricians and specialists who take developmental concerns seriously, and commit to early observation and early action if signs do appear. The post on early autism detection covers exactly why early identification and early support make such a significant difference to outcomes, and it is worth reading well before you need it.
What to Watch for in Your Children Early
If autism runs in your family, you are in an unusually strong position compared to most parents, because you already know what to watch for rather than discovering it through trial and error.
Key early signs worth monitoring closely given your family history include:
Limited response to their name being called by 12 months
Limited eye contact during everyday interaction and play
Delayed or absent babbling, words, or phrases at expected milestones
Loss of previously acquired language or social skills at any age
Strong preference for routine with significant distress at small changes
Repetitive movements such as hand flapping, rocking, or spinning
Intense, narrow interests that go well beyond typical childhood enthusiasm
Unusual responses to sounds, textures, lights, or other sensory input
Because if autism runs in your family you are already primed to notice these signs earlier than a parent with no family history might, use that advantage. Raise concerns with your pediatrician early and confidently, and do not let a single negative screening result fully settle your concerns if your gut is still telling you something is there.
Reading widely during this period also makes a real difference. Dropped in a Maze by Sonia Chand is one of the most honest accounts available of navigating the autism journey from the inside, written specifically for families who are finding their way through a system that does not always make it easy. If autism runs in your family and you are trying to build your understanding before you need it, or in the middle of needing it right now, this is the book to start with.
Get your copy of Dropped in a Maze
Talking to Family Members About a Possible Pattern
If autism runs in your family, conversations about it within the family are not always easy, particularly with older relatives who may have grown up in a generation where autism was poorly understood, heavily stigmatized, or simply never discussed.
A few things tend to help these conversations go better:
Lead with curiosity rather than diagnosis. Asking what was your childhood actually like opens doors that telling someone I think you were autistic tends to close.
Frame the conversation around understanding rather than labeling, particularly with relatives who may feel defensive about a retrospective diagnosis.
Share what you have learned about the genetics in a way that reduces shame rather than assigning blame. Nobody caused this. It is simply how genetics work.
Be patient. Some relatives will find this conversation freeing. Others will need time, or may never fully embrace it, and that is their right.
If autism runs in your family, these conversations, however they go, tend to build a richer and more compassionate understanding of your whole family across generations, not just the most recently diagnosed member.
What a Family History of Autism Does Not Mean
If autism runs in your family, it is worth being equally clear about what this does not mean, because misunderstanding the genetics can create unnecessary fear.
A family history of autism does not mean:
Every child you have will be autistic
Autism was caused by anything you did during pregnancy or in early parenting
Your family is somehow flawed or carries something to be ashamed of
Your child's life will be defined by limitation rather than possibility
You are guaranteed to recognize autism easily just because you have seen it before in your family
If autism runs in your family, what it actually means is that you have more genetic information than most families do, and that information is a tool for preparedness, not a sentence or a guarantee.
FAQs
If autism runs in your family, what are the chances your next child will be autistic?
Research estimates the recurrence rate for younger siblings at around 10 to 20 percent, significantly higher than the general population rate.
Can autism skip a generation?
Yes. Because autism involves many genetic variants rather than a single gene, it can appear to skip generations while still being present in the family's genetic background.
Can two non-autistic parents have an autistic child?
Yes. Autism can arise from spontaneous genetic mutations or from combinations of inherited variants that were not apparent in either parent individually.
Does having one autistic child mean future children will definitely be autistic?
No. The risk is elevated but not guaranteed. Most siblings of autistic children are not autistic themselves.
Final Thoughts
If autism runs in your family, you are looking at a genuine genetic pattern backed by decades of solid research, not a coincidence or an overreaction. Understanding what that pattern actually means, the real odds, the generational threads, and what to watch for, puts you in a stronger position than most families ever get to start from.
If autism runs in your family, let that knowledge work for you. Use it to advocate early. Use it to understand relatives, past and present, with more compassion. Use it to prepare rather than to fear. The thread running through your family is not something to be ashamed of. It is simply part of who your family is, and understanding it fully is the first step toward supporting every generation it touches.
References:
Wikipedia contributors. Heritability of autism [Internet]. Wikipedia, The Free Encyclopedia. Available from: https://en.wikipedia.org/wiki/Heritability_of_autism
Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). Science Update: Risk for autism spectrum disorder mainly influenced by genetics, suggests NICHD-funded study [Internet]. Available from: https://www.nichd.nih.gov/newsroom/news/080119-autism
Ozonoff S, Young GS, Bradshaw J, Charman T, Chawarska K, Iverson JM, Klaiman C, Landa RJ, McDonald N, Messinger D, Schmidt RJ, Wilkinson CL, Zwaigenbaum L. Familial Recurrence of Autism: Updates From the Baby
Siblings Research Consortium. Pediatrics. 2024;154(2):e2023065297. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11291960/
Talukdar M, Page DC. The inactive X chromosome as a female protector in autism and beyond. Res Sq [Preprint]. 2025 Sep 8:rs.3.rs-7539254. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12440103/

Is Autism an Intellectual Disability? What Parents Need to Know
Is autism an intellectual disability is one of the most commonly searched questions about autism and one of the most frequently misunderstood. Parents hear the term intellectual disability in the same conversation as their child's autism diagnosis and immediately wonder whether the two are the same thing, whether one causes the other, and what it means for their child's future.
Is autism an intellectual disability deserves a clear, direct answer because the confusion between the two has real consequences for how autistic children are seen, how they are supported, and what opportunities they are given access to.
This post answers the question is autism an intellectual disability honestly and completely, explains what both terms actually mean, looks at where they overlap and where they do not, and gives parents the practical information they need to advocate effectively for their child.
Table of Contents
Is Autism an Intellectual Disability?
What Is Autism?
What Is an Intellectual Disability?
Where Autism and Intellectual Disability Overlap
Where Autism and Intellectual Disability Differ
How Common Is Intellectual Disability in Autism?
Why Is Autism So Often Confused With Intellectual Disability?
The Problem With Assuming Intellectual Disability in Autism
How This Connects to Profound Autism
The Role of Coaching and Support
FAQs
Final Thoughts
Is Autism an Intellectual Disability?
Is autism an intellectual disability? No. Autism and intellectual disability are two separate conditions. They can co-occur in the same person but they are not the same thing and one does not cause the other.
Autism is a neurodevelopmental condition characterized by differences in social communication, sensory processing, and restricted or repetitive behaviors. Intellectual disability is a separate condition characterized by significant limitations in both intellectual functioning and adaptive behavior that originate before the age of 18.
Is autism an intellectual disability in the sense that autism always involves limited intellectual functioning? No. The majority of autistic people do not have an intellectual disability. Many autistic people have average, above average, or exceptional intellectual abilities.
Is autism an intellectual disability in the sense that intellectual disability and autism share some features? Yes, in limited ways. Both are neurodevelopmental conditions. Both are present from early childhood. And in some autistic individuals, both occur together. But having one does not mean having the other.
The confusion between the two is understandable given how frequently they are discussed together and how significantly intellectual disability affects the autism presentation when it is present. But the confusion has real costs when it leads to autistic children being underestimated, placed in inappropriate settings, or denied opportunities because someone assumed their autism meant intellectual disability.
What Is Autism?
Before going deeper into the question of is autism an intellectual disability, it helps to be clear about what each term actually means.
Autism, formally known as Autism Spectrum Disorder or ASD, is a neurodevelopmental condition that affects how a person communicates, processes information, experiences sensory input, and relates to others. It is present from birth and it is lifelong.
The core features of autism are:
Differences in social communication and social interaction across multiple contexts
Restricted, repetitive patterns of behavior, interests, or activities
Sensory processing differences that affect how the person experiences and responds to sensory input
Autism presents very differently across individuals. Some autistic people are nonverbal and require significant support across all areas of daily life. Others are highly verbal, academically capable, and manage many daily tasks independently. The spectrum is genuinely wide and the variability within it is enormous.
What autism does not inherently involve is limited intellectual functioning. Intellectual ability in autism ranges across the full spectrum from significant intellectual disability to exceptional intellectual gifts. Autism describes a neurological profile. It does not specify intelligence.
For a comprehensive understanding of what autism is at a neurological level and why the brain works differently in autistic people, the post on is autism a neurological disorder covers neuroscience in depth.
Dropped in a Maze, one of the bestselling books on Autism
What Is an Intellectual Disability?
Intellectual disability, formerly known as mental retardation in older clinical literature, is defined by three criteria that must all be present:
Significant limitations in intellectual functioning: An IQ score approximately two standard deviations below the mean, which typically means an IQ below 70, along with clinical judgment confirming significant cognitive limitations.
Significant limitations in adaptive behavior: Difficulty with the practical skills needed for everyday life including conceptual skills such as language and literacy, social skills such as interpersonal relationships and following rules, and practical skills such as personal care, managing money, and managing routines.
Onset during the developmental period: The limitations must be present before the age of 18, distinguishing intellectual disability from acquired cognitive impairments that develop in adulthood through injury or disease.
Intellectual disability ranges in severity from mild to moderate to severe to profound. The majority of people with intellectual disability, around 85 percent, have mild intellectual disability and can develop significant life skills with appropriate support.
Is autism an intellectual disability by this definition? No. Autism does not inherently involve significant limitations in intellectual functioning. An autistic person with an IQ of 120 has no intellectual disability. An autistic person with an IQ of 45 may have both autism and intellectual disability as co-occurring conditions.
Where Autism and Intellectual Disability Overlap
While is autism an intellectual disability has a clear no answer, autism and intellectual disability do overlap in some important ways that are worth understanding.
They can co-occur: Autism and intellectual disability are separate conditions but they frequently occur together in the same individual. Research suggests that somewhere between 30 and 40 percent of autistic people also have an intellectual disability. This co-occurrence is real and significant and it shapes the support needs and life experiences of those individuals in profound ways.
They are both neurodevelopmental: Both autism and intellectual disability are classified as neurodevelopmental conditions in the DSM-5. Both originate in differences in brain development during the prenatal and early postnatal period. Both are present from birth even when not identified until later.
They both affect learning: Both autism and intellectual disability can affect how a person learns, though they affect learning differently. Autism affects learning through differences in social communication, sensory processing, and information processing style. Intellectual disability affects learning through limitations in cognitive processing speed, working memory, and abstract reasoning.
They are both lifelong: Neither autism nor intellectual disability is something a person grows out of. Both are permanent aspects of the person's neurology. Support needs may change over time but the underlying conditions remain.
They both qualify for educational support: Both autism and intellectual disability qualify children for Individualized Education Programs under IDEA and for special education services. When they co-occur, the educational planning needs to address both conditions.
Where Autism and Intellectual Disability Differ
Understanding where autism and intellectual disability differ is just as important as understanding where they overlap, particularly when answering the question of is autism an intellectual disability.
Intellectual functioning: The most fundamental difference is that autism does not inherently involve limited intellectual functioning while intellectual disability does by definition. Autistic people can have IQs at any point on the full range of human cognitive ability.
Social communication: Autism specifically involves differences in social communication that are not explained by intellectual disability alone. An autistic person without intellectual disability has specific social communication differences that a person with intellectual disability of the same cognitive level would not necessarily have.
Sensory processing: Sensory processing differences are a core feature of autism and are not a defining feature of intellectual disability. Many autistic people have significant sensory sensitivities that profoundly affect their daily functioning in ways that are distinct from the challenges of intellectual disability.
Restricted and repetitive behaviors: The restricted and repetitive behaviors that characterize autism, including special interests, insistence on sameness, and repetitive movements, are not defining features of intellectual disability.
Cause: The genetic and neurological underpinnings of autism and intellectual disability differ significantly even though both involve differences in brain development. They represent distinct developmental pathways that happen to co-occur more frequently than chance would predict.
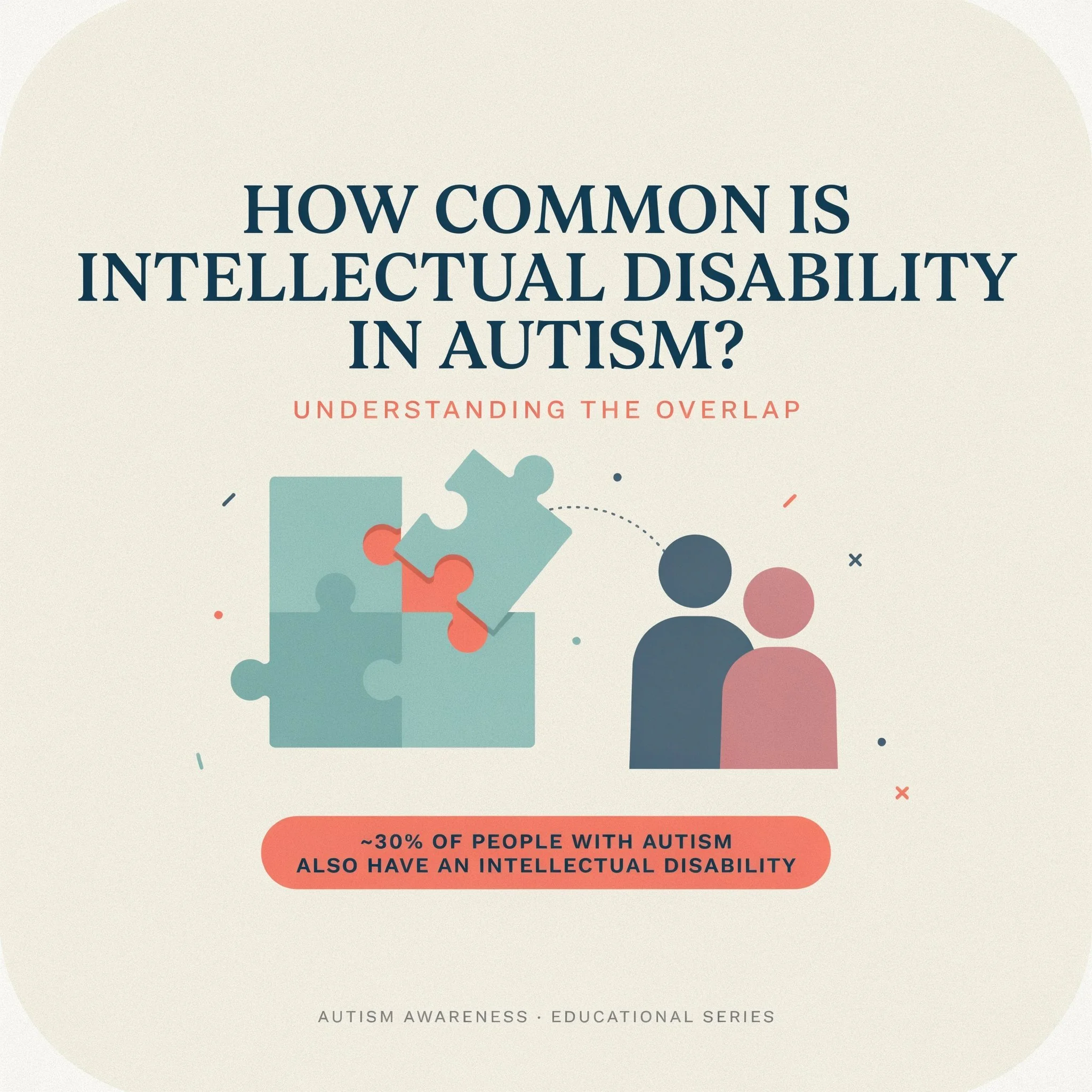
Common intellectual disability in autism
How Common Is Intellectual Disability in Autism?
The research on how common intellectual disability is in autism has produced varying estimates over the years, and understanding those variations helps parents make sense of conflicting information.
Earlier estimates suggested that around 70 to 75 percent of autistic people had intellectual disability. More recent research puts the figure significantly lower, at around 30 to 40 percent. This shift reflects several things.
First, diagnostic criteria for autism have broadened significantly since the 1990s, particularly with the inclusion of Asperger Syndrome in the DSM-4 and the subsequent shift to a single autism spectrum diagnosis in the DSM-5. The broader the diagnostic criteria, the more autistic people without intellectual disability are captured in prevalence data.
Second, better assessment tools have improved the accuracy of cognitive testing in autistic individuals. Earlier IQ assessments were often poorly adapted for autistic people, particularly those who were nonverbal or who had significant communication differences, and may have underestimated intellectual ability.
Third, awareness of autism without intellectual disability has increased significantly, leading to more diagnoses in this population and shifting the overall proportion.
The current best estimate is that approximately 30 to 40 percent of autistic people have a co-occurring intellectual disability. The majority, 60 to 70 percent, do not.
Why Is Autism So Often Confused With Intellectual Disability?
The confusion between autism and intellectual disability has several sources and understanding them helps parents recognize when assumptions are being made about their child that may not be accurate.
Historical reasons: Early autism research focused primarily on autistic individuals with significant support needs, many of whom also had intellectual disability. The image of autism that emerged from that research was heavily shaped by this population, creating an association between autism and intellectual disability that persisted long after research demonstrated the full breadth of the spectrum.
Communication differences: Many autistic children, particularly young autistic children and those who are nonverbal or minimally verbal, present in ways that can look like intellectual disability to observers who are not trained to distinguish the two. A child who does not respond to questions, who does not make eye contact, and who does not engage in typical social interaction may be assumed to have limited intelligence when the actual issue is communication and social differences, not cognitive limitation.
Assessment challenges: Standard intelligence tests are not always well-suited to autistic individuals. They typically require verbal responses, social engagement, and the ability to demonstrate knowledge through neurotypical channels. An autistic child who has significant knowledge and cognitive ability but cannot demonstrate it through standard testing channels may receive a lower IQ score than accurately reflects their ability.
Behavior misinterpretation: Autistic behaviors including limited eye contact, scripted language, repetitive movements, and unusual responses to social situations are sometimes misread as signs of intellectual limitation by people who do not understand autism.
The Problem With Assuming Intellectual Disability in Autism
This section matters as much as any other in this post because the assumption that is autism an intellectual disability translates to yes carries real and harmful consequences for autistic children.
When intellectual disability is assumed in an autistic child who does not have it, several things happen:
Educational placements become inappropriate: Children are placed in settings designed for intellectual disability rather than autism. The curriculum is pitched below their actual cognitive level. Expectations are lowered in ways that become self-fulfilling.
Communication is not pursued: When a child is assumed to have intellectual disability, the investment in finding their communication channel is often reduced. The assumption that they cannot communicate becomes the barrier to discovering that they can.
Strengths are overlooked: The deficit-focused lens of intellectual disability obscures the genuine cognitive strengths that many autistic people have. Pattern recognition, attention to detail, deep focused thinking, and exceptional memory in areas of interest are all common autistic cognitive profiles that are invisible when intellectual disability is assumed.
Self-concept is damaged: Children who are consistently treated as less capable than they are internalize that treatment. The damage to self-esteem and self-concept that comes from years of being underestimated is real, significant, and often persists long after the underestimation is corrected.
How This Connects to Profound Autism
The overlap between autism and intellectual disability is most significant at the most complex end of the autism spectrum. The concept of profound autism, which describes autistic individuals with both significant intellectual disability and minimal or no functional spoken language, is directly relevant to the question of is autism an intellectual disability.
For a full understanding of what profound autism is, how it differs from other autism presentations, and what support looks like for this population, the posts on what is profound autism and profound autism vs autism level 3 cover the topic comprehensively.
FAQs
Can you be autistic and have an intellectual disability?
Yes. Research suggests around 30 to 40 percent of autistic people have a co-occurring intellectual disability.
What percentage of autistic people have intellectual disability?
Current research estimates that approximately 30 to 40 percent of autistic people have a co-occurring intellectual disability meaning the majority do not.
Can an autistic child have a high IQ?
Yes. Many autistic people have average, above average, or exceptionally high IQ scores. High intelligence and autism are not mutually exclusive.
How is intelligence tested in autistic children? Standard intelligence tests are used alongside nonverbal assessments for children with communication differences. Subtest profiles are important because autistic children often show highly variable performance across different cognitive domains.
Does having autism mean my child will need lifelong support? Support needs in autism vary enormously. Some autistic people require minimal support as adults. Others need significant ongoing support. The presence or absence of intellectual disability is one factor among many that affects long-term support needs.
Final Thoughts
Is autism an intellectual disability? No. They are two separate conditions that can and do co-occur but that are distinct in their definitions, their neurological underpinnings, and their implications for support.
Understanding this distinction matters practically. It matters for how autistic children are assessed, how they are placed in educational settings, what expectations are held for them, and what opportunities are made available to them.
The assumption that is autism an intellectual disability answers yes has cost too many autistic people too many years of being underestimated, under-supported, and denied access to the cognitive and communicative channels that could have shown the world what they were actually capable of.
Your child's autism does not define their intelligence. Their autism defines how their brain is organized, how they process information, how they experience the world, and what kind of support they need to thrive in it. Those are very different things from intellectual ability, and treating them as the same thing is a mistake with consequences.
Know the difference. Advocate accordingly. And hold the highest genuinely appropriate expectations for your child at every stage of their journey.
References:
National Institute of Mental Health. Autism Spectrum Disorder [Internet]. Last reviewed December 2024. Available from: https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd
National Academies of Sciences, Engineering, and Medicine. Clinical Characteristics of Intellectual Disabilities. In: Boat TF, Wu JT, editors. Mental Disorders and Disabilities Among Low-Income Children. Washington (DC): National Academies Press (US); 2015. Available from: https://www.ncbi.nlm.nih.gov/books/NBK332877/
de Brito Wanderley D, Muratori F, Argollo N, Tolentino A, Miranda T, Vaz F, Campos V, Marques de Mattos A, Lucena R. Autistic Children and Adolescents Without Intellectual Disability: Individual and Family Profile. Clin Neuropsychiatry. 2025;22(3):215-228. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12302814/
Srivastava AK, Schwartz CE. Intellectual disability and autism spectrum disorders: causal genes and molecular mechanisms. Neurosci Biobehav Rev. 2014;46(2):161-174. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4185273/
Congressional Research Service. The Individuals with Disabilities Education Act (IDEA), Part B: Key Statutory and Regulatory Provisions [Internet]. Report R41833. Available from: https://www.congress.gov/crs-product/R41833
Russell G, Mandy W, Elliott D, White R, Pittwood T, Ford T. Selection bias on intellectual ability in autism research: a cross-sectional review and meta-analysis. Mol Autism. 2019;10:9. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6397505/
Autism Speaks. Autism diagnostic criteria: DSM-5 [Internet]. Available from: https://www.autismspeaks.org/autism-diagnostic-criteria-dsm-5

Early Autism Detection: What Happens When Autism Is Caught Early
Early autism detection is one of the most important factors in determining the quality of life an autistic child will go on to experience. When autism is caught early, the right support can be put in place during the period when the brain is most responsive to intervention, connections can be built before gaps become entrenched, and families can stop guessing and start understanding.
When autism is caught early, everything changes. Not because autism itself changes, the neurology is present from birth and it does not disappear with early identification, but because the environment around the child changes. The support arrives sooner. The misunderstandings are fewer. The years spent confused about why things feel so hard are replaced with years spent learning how to work with the brain your child has rather than against it.
This post covers what the research says about early autism detection, what early intervention actually involves, what parents should watch for, and why the question of when autism is identified matters as much as it does.
Table of Contents
What Early Autism Detection Actually Means
Why Timing Matters: What the Brain Research Says
What Happens When Autism Is Caught Early
Early Signs Parents Should Know
The Earliest Age Autism Can Be Detected
What Early Intervention Looks Like
Barriers to Early Autism Detection
What Parents Can Do Right Now
How Early Detection Connects to Acceptance
FAQs
Final Thoughts
What Early Autism Detection Actually Means
Early autism detection refers to the identification of autism during the earliest possible developmental window, ideally before the age of three and in many cases as early as 18 months. It is the process of recognizing the signs of autism, pursuing evaluation, receiving a diagnosis, and beginning appropriate support before the typical developmental period has passed.
Early autism detection does not mean catching something before it gets worse in the way that early cancer detection does. Autism is not a progressive disease. It does not get worse if it goes undetected. But the opportunities that early autism detection opens up are genuinely time-sensitive in ways that make the timing of identification practically significant.
Early autism detection matters because the brain of a young child is far more plastic and responsive to environmental input than the brain of an older child or an adult. The early years are when the neural connections that support communication, social engagement, sensory regulation, and learning are being most actively formed. When the right support is in place during that window, those connections develop in ways that serve the autistic child far better than they would without support.
Early autism detection is not about changing who an autistic child is. It is about giving their neurology the right conditions to develop as fully and as functionally as possible during the period when development is most responsive to those conditions.
Why Timing Matters: What the Brain Research Says
The neuroscience behind early autism detection is both compelling and straightforward. The brain of a child under three is undergoing a period of extraordinary development. Neural connections are being formed at a rate that will never be matched again in life. The brain is literally constructing itself based on the input it receives from the environment.
This is what neuroscientists call neuroplasticity, and it is at its most powerful in the earliest years of life. The practical implication for autism is significant: when the right support is introduced during this period, the developing brain can build more functional pathways for communication, social engagement, and sensory regulation than it would build without that support.
Research consistently demonstrates that children who receive early autism intervention, particularly before the age of three, show better outcomes across multiple domains including language development, social skills, adaptive functioning, and cognitive development compared to children who receive the same intervention later.
A study found that intensive early intervention significantly improved outcomes for autistic toddlers, with many children making gains that would not have been possible if intervention had begun at school age. Multiple subsequent studies have replicated and extended these findings.
This does not mean that intervention after the early years is ineffective. It absolutely is effective. But the window of maximum neurological responsiveness is real and early autism detection is what opens access to it.

Early autism intervention works
What Happens When Autism Is Caught Early
When autism is caught early the outcomes for autistic children are measurably better across nearly every domain that matters for long-term quality of life.
Language and communication: When autism is caught early and communication support begins during the critical language development window, children develop stronger functional communication skills. This includes both verbal language and alternative communication methods for children who are nonverbal. Early speech and language therapy can make a profound difference to a child's ability to communicate their needs, preferences, and experiences.
Social development: When autism is caught early, support can be tailored to help autistic children develop social skills and build relationships during the period when the social brain is most actively developing. This does not mean making autistic children perform neurotypical social behavior. It means helping them develop authentic ways of connecting with others that work with their neurology.
Sensory regulation: When autism is caught early, occupational therapy and sensory integration support can help children develop more effective sensory regulation strategies during the period when those strategies are most readily learned. Children who develop better sensory regulation early are less likely to experience the kind of sensory overload that significantly affects functioning at school and in the community.
Academic readiness: When autism is caught early, children enter school with more of the foundational skills they need to benefit from education. Communication, self-regulation, attention, and the ability to manage transitions all contribute to school readiness and all can be meaningfully supported through early intervention.
Family functioning: When autism is caught early, families understand what they are dealing with earlier. The confusion, the self-blame, the wondering what is wrong, and the misinterpretation of autistic behavior as intentional or willful all reduce when there is a diagnosis and a framework for understanding the child. Families can access support, connect with community, and build their own knowledge and confidence much sooner.
Mental health: When autism is caught early, the years of struggling without understanding are shorter. Many autistic adults who were diagnosed late report significant mental health impacts from years of not understanding why they were different and why things that seemed easy for others felt so hard. Early autism detection reduces the duration of that confusion.
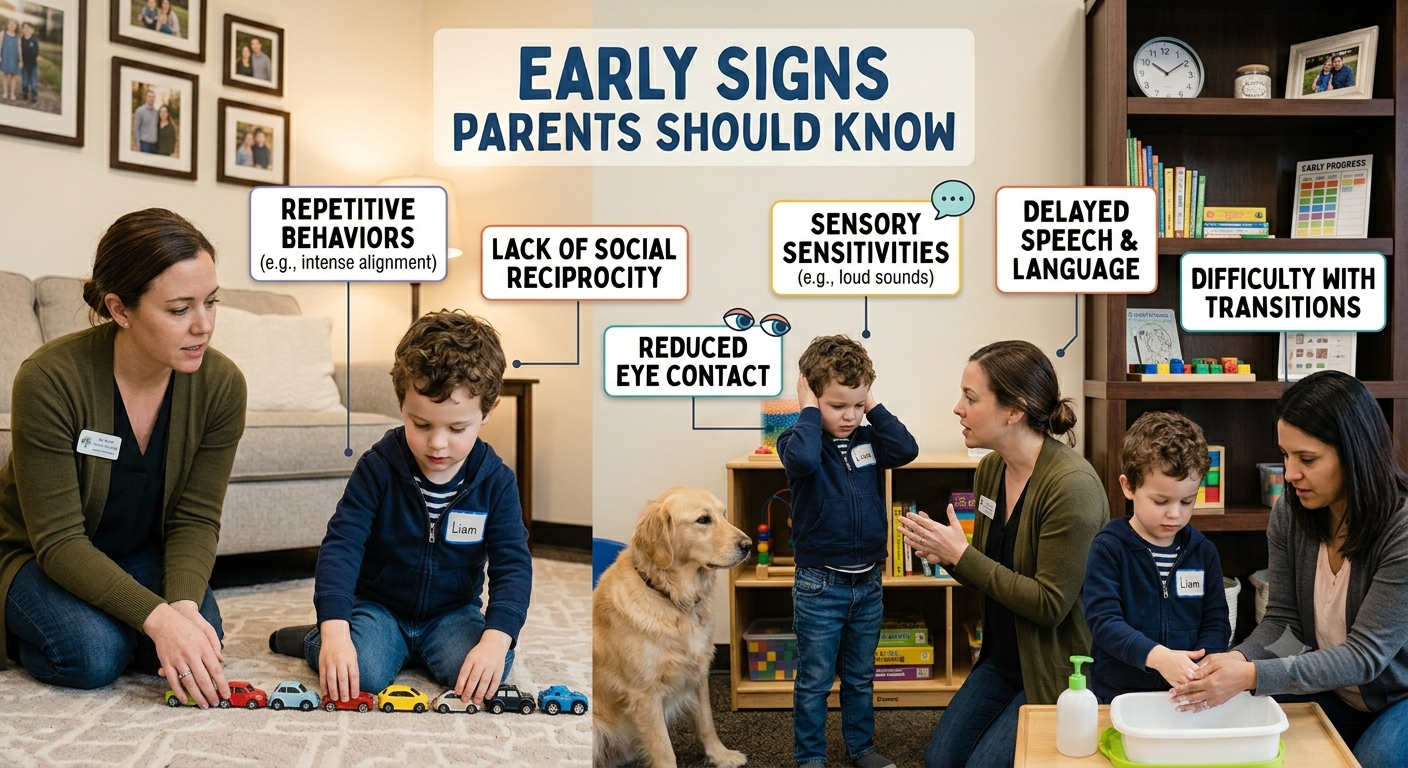
Autism Signs
Early Signs Parents Should Know
Knowing the early signs of autism is part of early autism detection and it is something every parent benefits from understanding whether or not they currently have concerns about their child.
Signs in the first year:
Limited eye contact during feeding and social interaction
Not responding to their name by 9 to 12 months
Not showing things to parents by pointing by 12 months
Limited babbling or loss of babbling that had been developing
Not reaching toward familiar people
Unusual responses to sensory input including sounds, touch, or lights
Signs between 12 and 24 months:
Not using single words by 16 months
Not using two-word phrases by 24 months
Loss of previously acquired language at any point
Not engaging in simple pretend play by 18 months
Limited interest in other children
Strong preference for specific routines with significant distress at changes
Repetitive movements including hand flapping, spinning, or rocking
Intense focus on specific objects or aspects of objects
Signs in the preschool years:
Significant difficulty with peer interaction
Unusual language patterns including echolalia, scripted speech, or very formal language
Extreme reactions to sensory input
Intense, narrow interests that dominate play
Difficulty with transitions and unexpected changes
Limited pretend play or play that is highly repetitive
The presence of any of these signs does not confirm autism. But it does mean that seeking evaluation is the right next step. For a complete guide to the testing process once concerns have been identified, the post on how to test for autism covers every stage in detail.

Ages autism can be detected
The Earliest Age Autism Can Be Detected
Early autism detection has its limits, and those limits are worth understanding honestly.
The American Academy of Pediatrics recommends autism-specific screening at 18 and 24 months. Research suggests that reliable autism identification is possible from around 18 months for children showing clear signs and from 24 months for more subtle presentations.
Some research has found that certain early markers in infant behavior, including patterns of eye contact, response to name, and social engagement, can be detectable as early as six months in infants who are later diagnosed with autism. These very early markers are currently the subject of active research but are not yet used in routine clinical screening.
For most families, the realistic window for early autism detection begins between 18 and 24 months when standard screening tools are reliable and diagnostic evaluations can be conducted with confidence.
It is worth noting that even an 18 to 24 month diagnosis, while considered early in clinical terms, still allows access to early intervention services during the most critical developmental window. Early is relative, and any diagnosis before school age opens doors that later diagnosis does not.
For parents who are carrying the emotional weight of a new diagnosis and trying to find their footing between the urgency of early intervention and the importance of acceptance, Sonia's coaching work is built for exactly that balance.
Book a coaching session with Sonia here and get the support that helps you hold both the urgency and the acceptance at the same time.
What Early Intervention Looks Like
Early autism detection is only valuable if it is followed by early intervention. Understanding what early intervention actually involves helps parents know what to pursue and what to expect.
Speech and language therapy: Communication support is almost universally recommended as part of early intervention for autistic children. This includes verbal language development for children who are developing speech and AAC implementation for children who are nonverbal or minimally verbal. Early speech therapy during the critical language development window is one of the most impactful interventions available.
Occupational therapy: Occupational therapy in early intervention addresses sensory processing, fine motor development, and the daily living skills that autistic children may need specific support to develop. Sensory integration approaches help young autistic children develop more effective regulation strategies during the period when those strategies are most readily learned.
Applied Behavior Analysis: ABA therapy is widely used in early autism intervention and has the most extensive evidence base of any autism intervention approach. It is also the most debated, with significant concerns raised by autistic advocates about historical ABA practices focused on compliance and suppression of autistic traits. Modern naturalistic ABA approaches that focus on skill development in the context of play and child-led interaction are generally considered more appropriate than older discrete trial formats.
Developmental relationship-based approaches: Approaches including DIR Floortime and the Early Start Denver Model use child-led play and relationship-based interaction to support communication, social engagement, and development. These approaches have growing evidence bases and are widely endorsed by autistic advocates as more affirming than purely behavioral approaches.
Early childhood special education: Many children with early autism detection qualify for early childhood special education services through their school district beginning at age three. These services provide structured educational support in settings designed for children with developmental needs.
Parent coaching: One of the most impactful components of early intervention is supporting parents to understand their child's communication and developmental needs and to respond in ways that promote development in everyday interactions. Parent coaching multiplies the impact of formal therapy by extending support into every interaction throughout the child's day.
Barriers to Early Autism Detection
Early autism detection is not equally available to all families and the barriers that prevent it are worth naming clearly.
Racial and ethnic disparities:Research consistently shows that Black, Hispanic, and Asian children are diagnosed with autism later on average than white children. These disparities reflect systemic inequities in access to healthcare, cultural factors that affect how autistic behavior is interpreted, and bias in the referral and diagnostic process.
Geographic barriers: Families in rural and remote areas often face significant barriers to autism evaluation including limited availability of specialist services and long travel distances to evaluation centers.
Economic barriers: Comprehensive private autism evaluations can cost several thousand dollars. Public pathways exist but have long waiting lists in many areas. Families without resources to access private evaluation may wait significantly longer for diagnosis.
Cultural barriers: In some communities, autism is stigmatized in ways that prevent families from seeking evaluation. Cultural beliefs about the cause of developmental differences, distrust of medical systems, and concerns about labeling can all delay early autism detection.
Professional barriers: Not all pediatricians are equally knowledgeable about autism. Concerns raised by parents are sometimes dismissed, minimized, or attributed to parenting anxiety. Families of girls are particularly likely to encounter this barrier.
Addressing these barriers is a systemic issue that goes beyond what individual families can solve. But knowing they exist helps parents advocate more effectively when they encounter them.
What Parents Can Do Right Now
If you are concerned about your child's development, here is what to do:
Request autism screening at your child's next pediatric appointment, or sooner if concerns are present
Document specific behaviors you have observed with dates and contexts
Request a referral for a full autism evaluation if screening raises concerns or if you have concerns regardless of screening results
Contact your local early intervention program directly if your child is under three, you do not need a referral in most states
Request a free educational evaluation through your school district if your child is three or older
Connect with other autism families who can share their experience navigating the evaluation and early intervention process
How Early Detection Connects to Acceptance
Early autism detection is most valuable when it is followed not just by early intervention but by early acceptance.
The goal of early identification is not to minimize autism or to engineer the most neurotypical version of the autistic child possible. It is to understand the child deeply enough, early enough, to build a life and an environment that genuinely supports them.
That requires acceptance alongside intervention. Acceptance of the autistic neurology as the genuine, permanent, valuable foundation of who your child is. Acceptance that the goal is flourishing as an autistic person, not passing as a neurotypical one.
The post on autism awareness vs autism acceptance covers why that distinction matters and what acceptance looks like in practice. It is worth reading early in the journey because the framework you bring to your child's diagnosis shapes every decision you make from here.
FAQs
What does it mean when autism is caught early
Early autism detection means identifying autism before age three when the brain is most responsive to intervention and support can be put in place during the critical developmental window.
What happens when autism is caught early?
When autism is caught early children show better outcomes in communication, social development, sensory regulation, school readiness, and mental health compared to children identified later.
Can autism be detected at birth?
Not reliably. Early markers may be present in the first months of life but reliable identification typically begins around 18 months using validated screening tools.
Does early detection mean early intervention always works? Early intervention significantly improves outcomes but results vary depending on the individual child, the type of intervention, and the quality of support provided.
What is the best early intervention for autism?
No single approach works for every child. Speech therapy, occupational therapy, developmental relationship-based approaches, and parent coaching all have strong evidence bases for early intervention.
Does early autism detection change the autism itself?
No. Autism is neurological and present from birth. Early detection changes the support environment, not the underlying neurology.
Does early autism detection prevent autism regression?
Early detection and appropriate support reduce the risk of autism regression by building stronger regulatory and communicative foundations before the demands that trigger regression become significant.
Final Thoughts
Early autism detection is not about fear. It is not about catching something terrible before it gets worse. It is about giving an autistic child the right conditions at the right time, during the window when those conditions make the most difference to how their brain develops and how their life unfolds.
When autism is caught early, families stop guessing and start understanding. Children stop struggling in silence and start receiving support that makes sense of their experience. The years of confusion are shorter. The foundation is stronger. The path forward is clearer.
If you have concerns about your child's development, act on them now. The evaluation process is navigable. The early intervention services are accessible. And the difference that early autism detection makes to a child's life is real, measurable, and worth every step of the process it takes to get there.
Your child's brain is working hard. Early autism detection is how you make sure the world works with it.
References:
Maksimović S, Marisavljević M, Stanojević N, Ćirović M, Punišić S, Adamović T, Đorđević J, Krgović I, Subotić M. Importance of Early Intervention in Reducing Autistic Symptoms and Speech–Language Deficits in Children with Autism Spectrum Disorder. Children (Basel). 2023 Jan 6;10(1):122. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9857540/
Estes A, Munson J, Rogers SJ, Greenson J, Winter J, Dawson G. Long-Term Outcomes of Early Intervention in 6-Year-Old Children With Autism Spectrum Disorder. J Am Acad Child Adolesc Psychiatry. 2015 Jul;54(7):580-7. Available from: https://pubmed.ncbi.nlm.nih.gov/26088663/
American Academy of Pediatrics. Autism Spectrum Disorder [Internet]. Last updated October 2025. Available from: https://www.aap.org/en/patient-care/autism/
Young GS, Merin N, Rogers SJ, Ozonoff S. Gaze Behavior and Affect at 6-Months: Predicting Clinical Outcomes and Language Development in Typically Developing Infants and Infants At-Risk for Autism. Dev Sci. 2009 Sep;12(5):798-814. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2732664/
International Council on Development and Learning (ICDL). What is DIR®? [Internet]. Available from: https://www.icdl.com/dir
Autism Speaks. What is Early Start Denver Model (ESDM)? [Internet]. Available from: https://www.autismspeaks.org/early-start-denver-model-esdm
Aylward BS, Gal-Szabo DE, Taraman S. Racial, Ethnic, and Sociodemographic Disparities in Diagnosis of Children with Autism Spectrum Disorder. J Dev Behav Pediatr. 2021 Oct-Nov;42(8):682-689. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8500365/